
When Calcium Scoring Helps vs. When It Misleads
The Real Power of Zero (and Why It Doesn’t Last Forever)

“CAC has revolutionised CV prevention...” - Peter Attia’s recent tweet caught my attention. He’s right that calcium scoring transformed risk assessment.
I got to read extensively about coronary artery calcium over the last few weeks, and I can tell you the reality is more nuanced. When used in the right patients, CAC is the single best test we have for determining who actually needs aggressive heart disease prevention—it changes treatment decisions in nearly half of people who get it. But it doesn’t work equally well for everyone, and a zero score doesn’t mean you’re immune from heart disease.
In this newsletter, I’ll walk you through when CAC meaningfully changes management versus when it offers false reassurance.
1. The power and limits of a zero calcium score
CAC=0 represents the strongest negative predictor we have in cardiovascular medicine, but this protection comes with an expiration date.
In people without symptoms, annual heart attack rates with CAC=0 average 0.027%—translating to 99.4% survival over 10 years¹. The CAC Consortium tracked thousands of individuals and found death rates of only 0.32 to 0.43 per 1,000 person-years when calcium was absent.¹ These numbers explain why many cardiologists call it the “power of zero.”
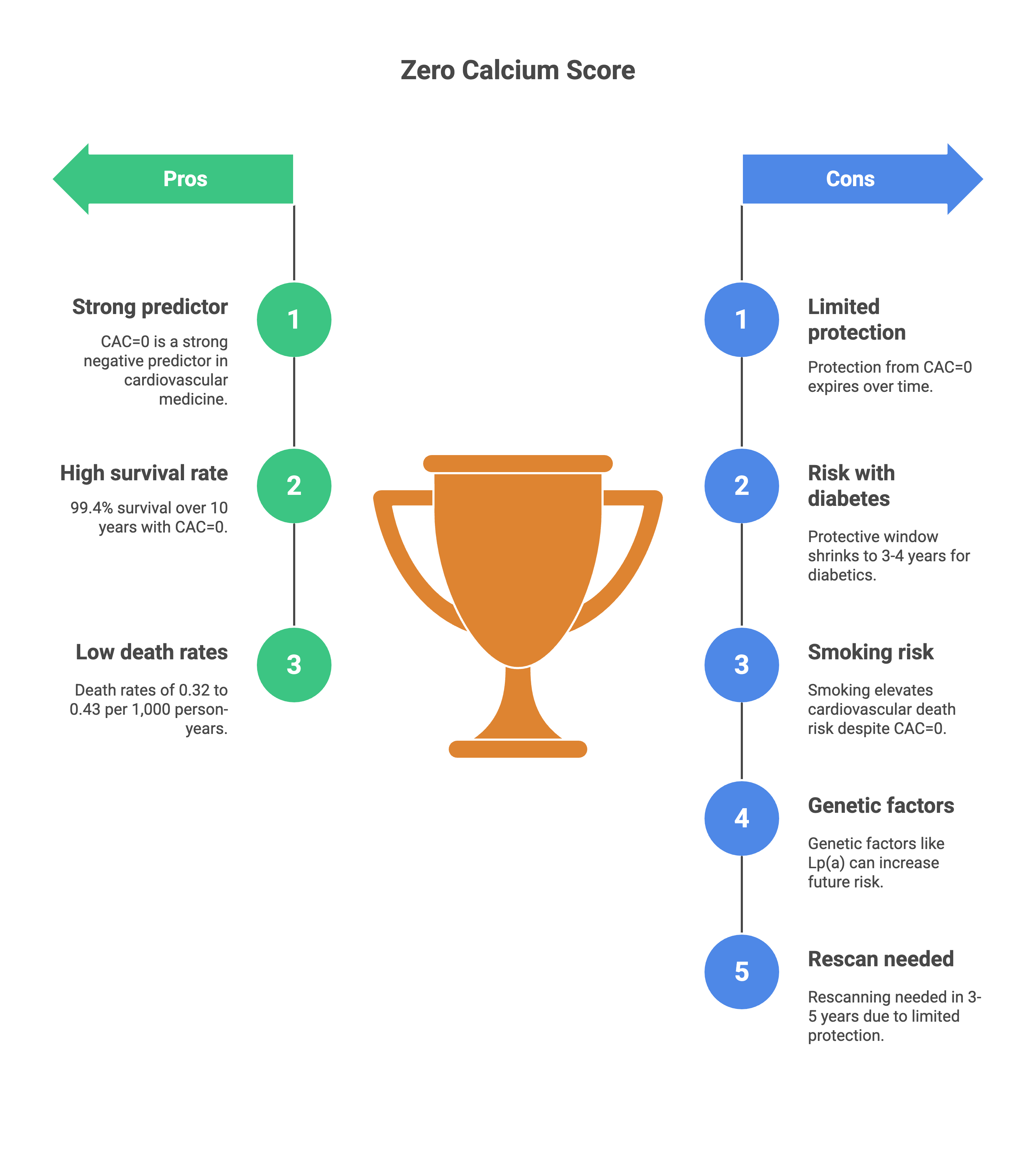
But this warranty period shortens dramatically depending on your risk profile. If you have diabetes, that protective window shrinks to just 3-4 years compared to 5-7 years for non-diabetics.² The Multi-Ethnic Study of Atherosclerosis revealed that women with diabetes maintain CAC=0 protection for 4.3 years versus 6.9 years without diabetes. For men with diabetes, the warranty drops to 3.1 years compared to 4.8 years². The message: if you have diabetes and get a zero score, you’ll need another scan in 3 years rather than waiting the typical 5 years.
Current smokers with CAC=0 face a particularly striking risk elevation—2.10 times higher cardiovascular death rates compared to nonsmokers with zero calcium.³ That risk level matches what nonsmokers experience when their calcium scores reach 100-399. The “power of zero” essentially evaporates if you continue smoking.
A common scenario that illustrates the complexity
Last week, I wrote a thread on Lp-a, and someone posted this in reply
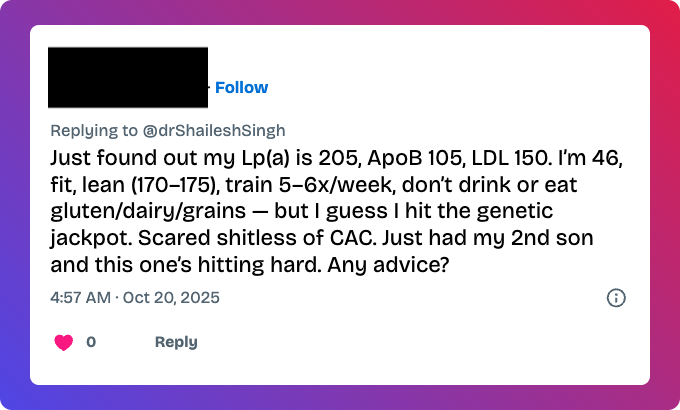
This captures the exact anxiety many people face when they discover elevated Lp(a)—a genetic risk factor they can’t diet or exercise away. The question becomes: should he get a calcium score, and what would it actually tell him?
Two recent studies clarified how Lp(a) and calcium scores interact in ways that challenge what many people assume. A 2025 study in the Journal of Clinical Lipidology examined how these markers predict atherosclerotic cardiovascular disease.⁴ High Lp(a) alone carried an odds ratio of 1.36 for prevalent disease, while positive calcium scoring showed an odds ratio of 1.79. When both were elevated together, the odds ratio jumped to 2.40.
But here’s what matters for this person’s immediate question: high Lp(a) with CAC=0 did NOT significantly increase the odds for cardiovascular disease.⁴
The 2022 JACC analysis of 6,590 participants showed something similar.⁵ Elevated Lp(a) increased cardiovascular risk overall, but among those with CAC=0, elevated Lp(a) failed to stratify near-term risk further. The multiplicative effect only emerged when both markers were elevated—patients with Lp(a) in the highest quintile AND calcium scores exceeding 100 had 10-year risk above 15%, while those with low Lp(a) and CAC=0 stayed below 2%.⁵
These findings reveal something fundamental: Lp(a) and calcium measure different things. Roughly 25% of patients with CAC=0 have Lp(a) exceeding 40 mg/dL, and 15% maintain zero calcium despite Lp(a) above 40.⁵ Lp(a) predicts who will develop atherosclerosis in the future, while calcium measures who already has established disease right now.
For this 46-year-old, a zero calcium score would mean his current risk remains low despite the genetic predisposition—likely low enough to defer statins while maintaining aggressive lifestyle management. But the elevated Lp(a) means atherosclerosis development continues in the background, making rescanning in 3-5 years critical to catch disease before it becomes clinically significant.
The most important limitation: among patients with CAC=0 followed in MESA, 19% of all coronary events over 10 years occurred before the recommended 3-5 year rescan window.⁶ Zero calcium provides time-limited reassurance, not lifetime immunity.
2. What CAC detects versus what it misses
Here’s what you need to understand about calcium scoring: it only shows you the calcified part of plaque buildup. Calcium represents roughly one-fifth of total plaque burden, and this limitation changes how useful the test is depending on your age and symptoms.
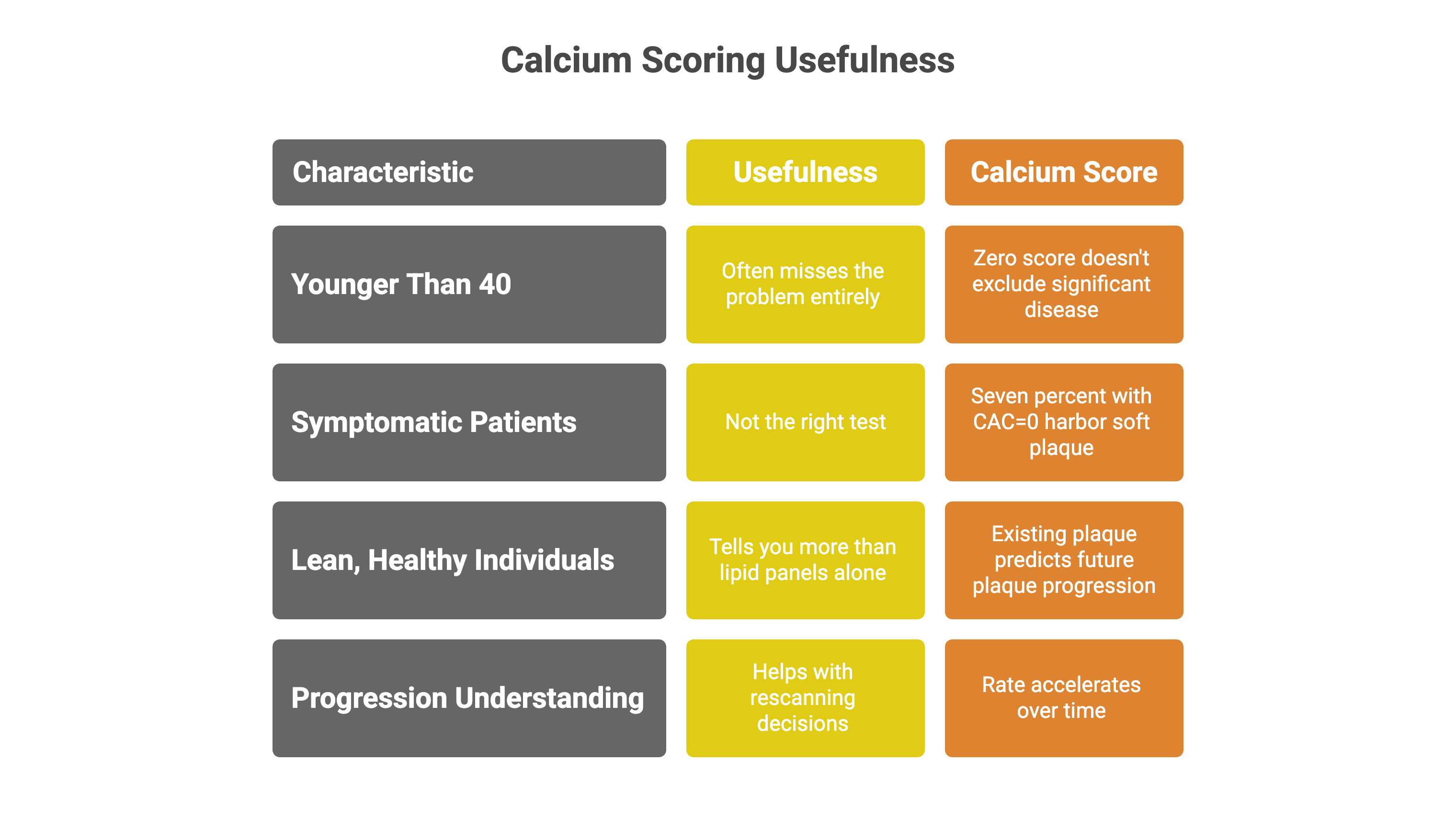
If you’re younger than 40, calcium scoring often misses the problem entirely. Among patients under 40 with serious coronary blockages, 58% have zero calcium compared to only 5% of those over 70.⁷ Young adults develop soft, non-calcified plaque that takes decades to calcify. A zero score in your 30s doesn’t exclude significant disease—it just means the disease hasn’t been there long enough to turn into calcium yet. This explains why calcium scoring works poorly for early detection in younger populations.
If you have symptoms—chest pain, shortness of breath, unusual fatigue—calcium scoring isn’t the right test. You need imaging that shows the actual blockages, not just calcium deposits. Seven percent of symptomatic patients with CAC=0 harbor significant soft plaque when you look with more detailed imaging.⁸ South Asian populations show even higher rates—28.8% demonstrate soft plaque despite zero calcium, including some with blockages exceeding 50%.⁹ If you’re experiencing symptoms, your physician should order tests that visualize the full picture of your coronary arteries, not just the calcified portions.
Once calcium appears, understanding how it progresses helps with rescanning decisions. On average, calcium scores increase 20-25% annually, though individual patterns vary widely.¹⁰ Among 3,116 people with initially zero calcium followed for 10 years, about half developed detectable calcium, roughly one-third progressed to scores above 10, and nearly one in ten reached scores exceeding 100.¹¹ The rate accelerates over time—2-3% per year in the first two years, climbing to 4-5% per year between years 4-10.¹¹
What this means practically: if your first calcium score comes back at zero, your risk of developing significant calcium (scores above 100 that change treatment recommendations) within 3-5 years runs below 10%. But that probability increases the longer you wait between scans, which is why the warranty period concept matters. A zero score today doesn’t prevent calcium accumulation tomorrow.
Something unexpected from the progression data: how fast your calcium grows matters less than where it stands right now. Your most recent absolute calcium score predicts future cardiovascular events better than knowing whether you progressed rapidly or slowly.¹² This suggests focusing on your current disease burden rather than obsessing over whether last year’s score of 50 jumped to 75 or crept to 60.
For lean, metabolically healthy individuals with elevated lipids but no obesity, metabolic syndrome, or insulin resistance, calcium scoring likely tells you more than lipid panels alone. A trial of 100 lean subjects with BMI below 25 and LDL cholesterol between 200-600 mg/dL found that existing plaque predicted future plaque progression over 12 months while LDL-C and ApoB levels did not.¹³ In this specific phenotype, knowing whether atherosclerosis already exists appears more important than measuring cholesterol particle concentrations.
3. When CAC creates clarity versus when it misleads
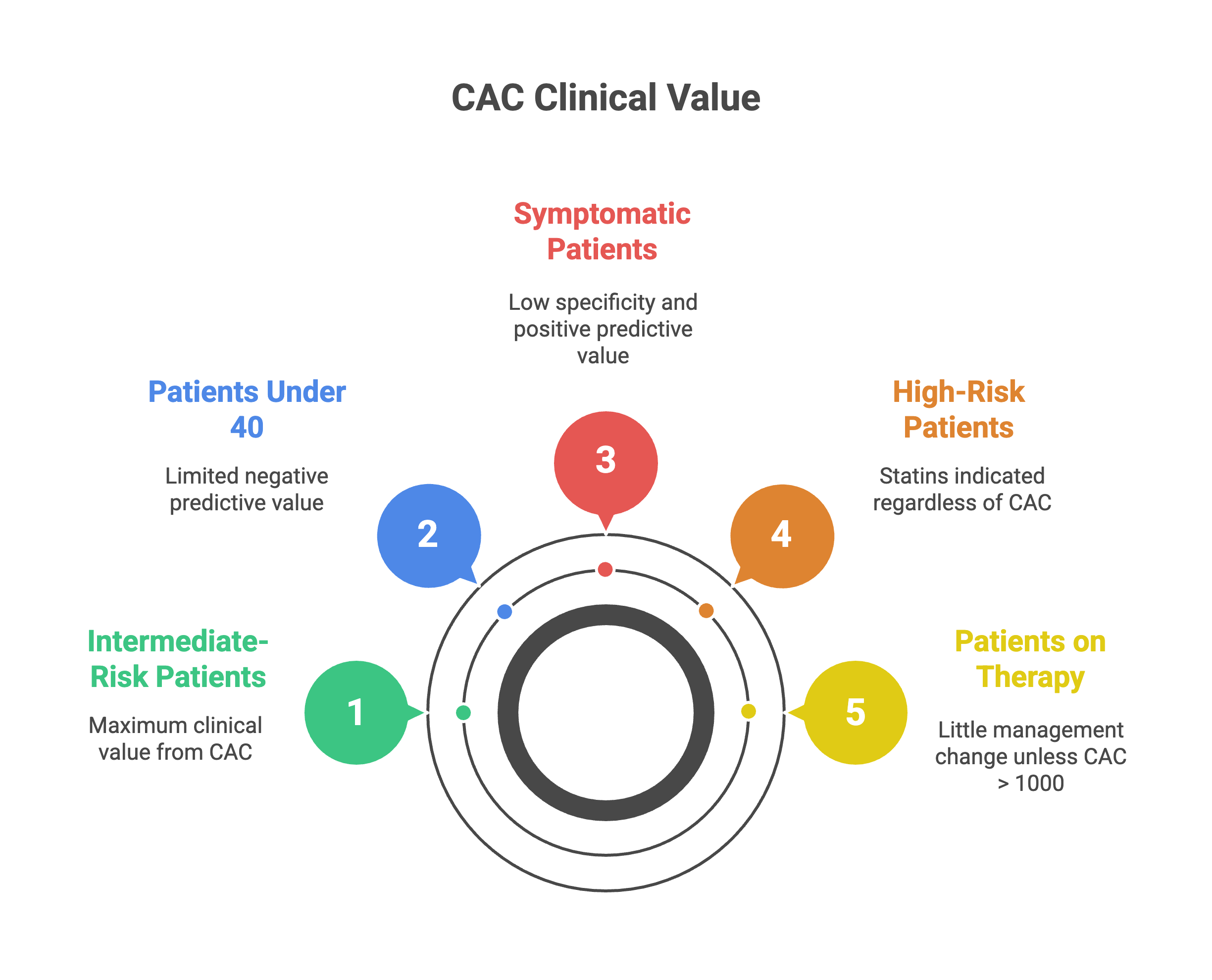
CAC provides maximum clinical value in a precisely defined population: intermediate-risk primary prevention patients aged 40-75 where treatment decisions remain genuinely uncertain after considering all other factors.
Here’s where calcium scoring actually changes decisions: In studies of people with intermediate risk—those genuinely uncertain about whether to start statins—about half get a zero calcium score.¹⁴ For these people, their near-term heart attack and stroke risk runs low enough that deferring medications makes sense while focusing on lifestyle.
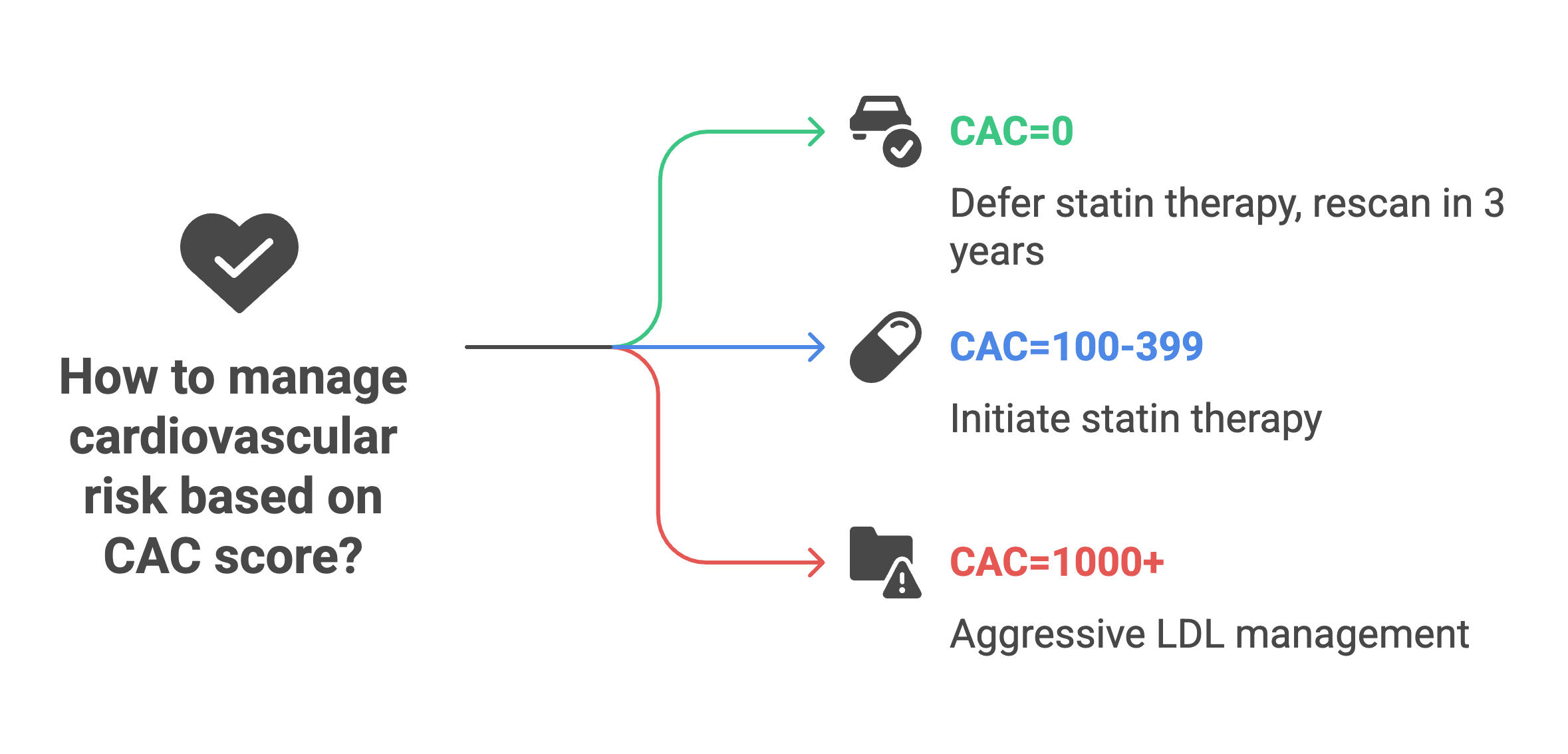
The other half discover they have calcium, and this is where the conversation shifts. About one in four to one in three people find their calcium scores exceed 100, revealing enough established disease that starting medications becomes clearly beneficial—not based on risk calculators or theoretical models, but because you can see the atherosclerosis already present in your arteries.¹⁴ The test essentially splits people who thought they were in a gray zone into two clearer groups: those who can reasonably wait on medications, and those who have enough disease that medications offer tangible benefit.
Several populations derive limited or misleading information from calcium scoring. Patients under age 40 show that 58% with obstructive coronary disease have CAC=0—the test’s negative predictive value collapses in young adults whose atherosclerosis remains predominantly non-calcified.⁷ Symptomatic patients require functional or anatomic assessment beyond calcium quantification because calcium scoring shows only 40% specificity and 68% positive predictive value for obstructive disease when symptoms are present.¹⁵ Very high-risk patients with 10-year cardiovascular risk exceeding 20% already have indications for statins regardless of what calcium scoring shows. Patients already on maximal preventive therapy gain little from confirming plaque burden that won’t change management unless calcium exceeds 1,000, which might prompt consideration of PCSK9 inhibitors.¹⁶
The resolution for someone with well-controlled diabetes, lifestyle-managed dyslipidemia, high Lp(a), lean BMI, regular exercise, and preference for evidence over reflexive pharmaceutical intervention comes down to three specific scenarios. A score of zero would justify deferring statin therapy despite diabetes and high Lp(a), though rescanning in 3 years remains appropriate given these risk factors shorten the warranty period to 3-4 years. The new data from JACL 2025 clarifies that high Lp(a) with CAC=0 doesn’t increase near-term risk—calcium presence matters more than atherogenic particle concentration for immediate management decisions.⁴
A score of 100-399 would clearly indicate statin benefit with numbers needed to treat ranging from 46-84, potentially overcoming pharmaceutical skepticism through visualization of established disease rather than theoretical risk calculations.¹⁷ A score of 1,000 or higher would establish very-high-risk status warranting LDL cholesterol targets below 55 mg/dL and consideration of PCSK9 inhibitors if targets remain unmet despite statins plus ezetimibe.¹⁶
4. Addressing two critical misconceptions
Misconception 1: CAC should be universal screening for all adults
Online advocates claim calcium scoring should replace traditional risk assessment for everyone, citing superior predictive accuracy and the “power of zero.” This position misreads what the evidence actually supports.
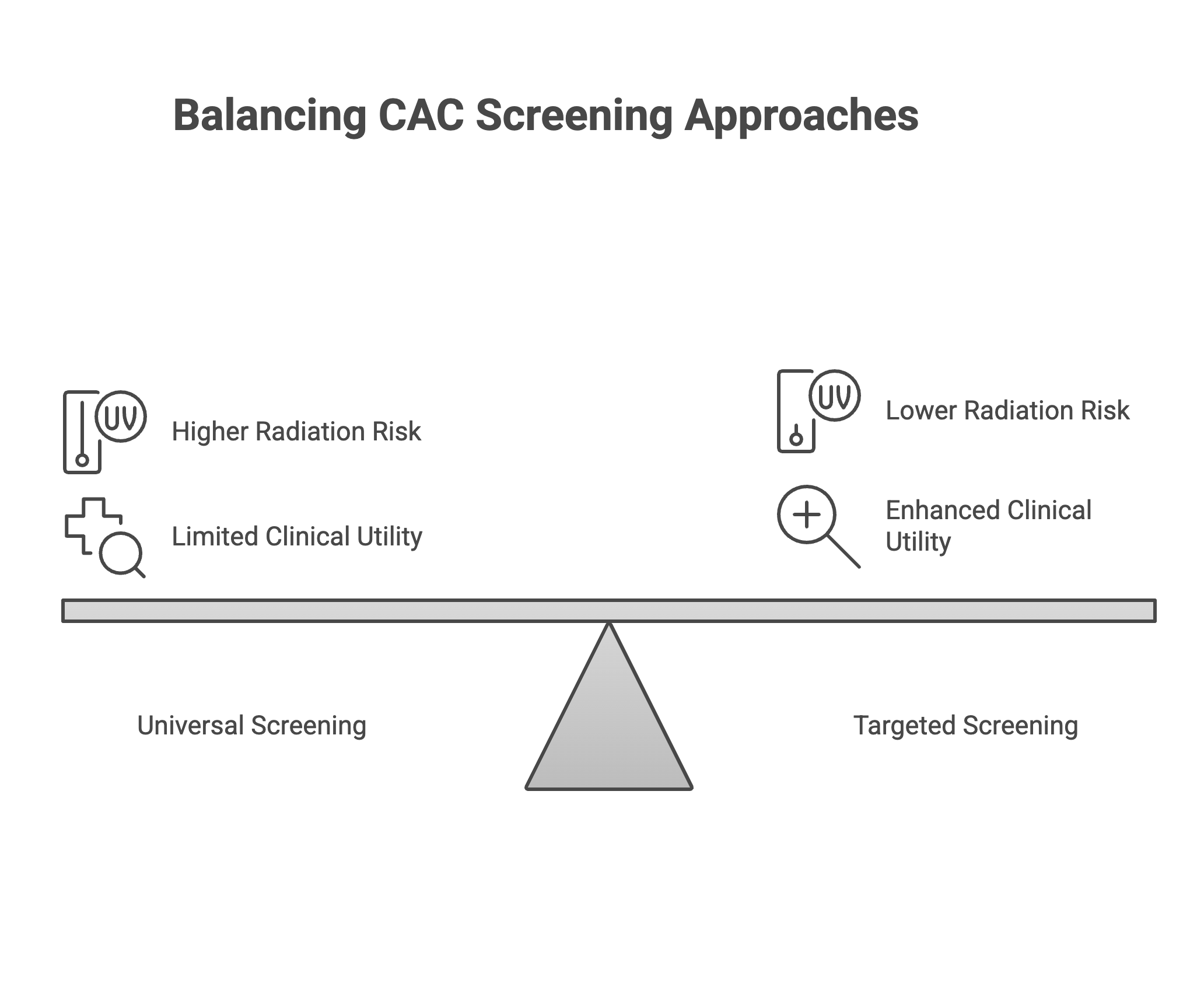
CAC functions as precision medicine for cardiovascular prevention in intermediate-risk populations where treatment decisions lack clarity, not as universal screening replacing clinical judgment. The biomarker works best when clinical uncertainty exists—when you and your physician genuinely aren’t sure whether starting preventive medications makes sense based on other factors. For someone already at high risk with clear medication indications, calcium scoring just confirms what we already know. For someone at very low risk, the test rarely changes management because preventive medications weren’t indicated anyway.
The radiation exposure argument against universal screening holds less weight than critics claim. Modern scanning protocols deliver approximately 1 mSv of radiation—equivalent to four months of natural background exposure.¹⁸ The estimated lifetime cancer risk from this radiation dose runs between 1-2 cancers per 100,000 scanned individuals.¹⁸ This risk sits substantially lower than the diagnostic benefit of accurate risk reclassification in 30-40% of appropriately selected patients. But radiation becomes less justifiable when applied to populations where the test won’t change management decisions.
Misconception 4: CAC=0 means lifetime immunity from heart disease
The zero score provides powerful reassurance, but treating it as lifetime immunity misunderstands how atherosclerosis develops over time.
In asymptomatic populations, CAC=0 delivers 99.4% 10-year survival with annual coronary event rates averaging 0.027%.¹ These numbers justify calling zero calcium a “warranty” against near-term cardiovascular events. But warranty periods have expiration dates that depend on your other risk factors.
For people with diabetes, that warranty runs 3-4 years rather than the 5-7 years seen in non-diabetics.² Current smokers with CAC=0 face 2.10-fold increased cardiovascular mortality compared to nonsmokers with zero calcium—risk equivalent to nonsmokers with calcium scores between 100-399.³ High Lp(a) combined with other risk factors drives ongoing atherosclerosis development even when today’s calcium score shows zero.
The Multi-Ethnic Study of Atherosclerosis revealed that 19% of all 10-year coronary events in CAC=0 patients occurred before the recommended 3-5 year rescan.⁶ Among 3,116 MESA participants with baseline CAC=0 followed for 10 years, 53% developed detectable calcium, 36% progressed to scores above 10, and 8% reached scores exceeding 100.¹¹ Zero calcium today doesn’t prevent calcium accumulation tomorrow—it just tells you where you stand right now.
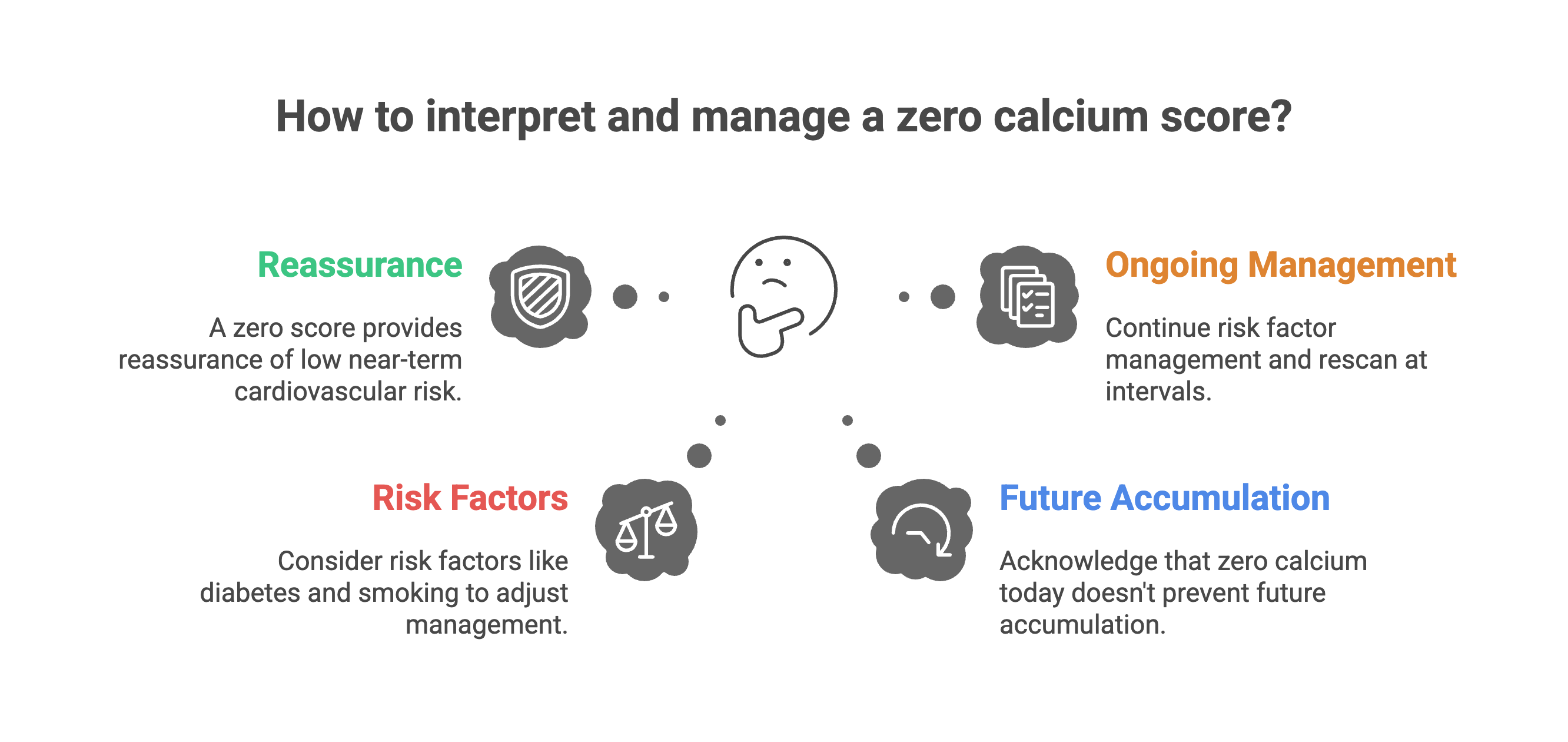
The appropriate interpretation: CAC=0 indicates current low risk that justifies deferring preventive medications in many situations, but ongoing risk factor management remains critical, and rescanning at appropriate intervals based on your risk profile ensures the zero score hasn’t changed to something that would alter treatment decisions.
If you found this useful, please share it.
Evidence over opinions. Clarity over noise. That’s Signal Over Noise.
References
Blaha MJ, Cainzos-Achirica M, Greenland P, et al. Role of coronary artery calcium score of zero and other negative risk markers for cardiovascular disease: the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation. 2016;133(9):849-858.
Malik S, Zhao Y, Budoff M, et al. Coronary artery calcium score for long-term risk classification in individuals with type 2 diabetes and metabolic syndrome from the Multi-Ethnic Study of Atherosclerosis. JAMA Cardiol. 2017;2(12):1332-1340.
McEvoy JW, Blaha MJ, DeFilippis AP, et al. Coronary artery calcium progression: an important clinical measurement? A review of published reports. J Am Coll Cardiol. 2010;56(20):1613-1622.
Park HE, Kim M, Choi SY. Association of lipoprotein(a) and coronary artery calcium with atherosclerotic cardiovascular disease. J Clin Lipidol. 2025;19(2):e234-e242.
Mehta A, Rigdon J, Tattersall MC, et al. Association of lipoprotein(a) and coronary artery calcium score for predicting cardiovascular disease events in adults (from the Multi-Ethnic Study of Atherosclerosis [MESA]). Am J Cardiol. 2022;150:1-8.
Nasir K, Bittencourt MS, Blaha MJ, et al. Implications of coronary artery calcium testing among statin candidates according to American College of Cardiology/American Heart Association Cholesterol Management Guidelines: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2015;66(15):1657-1668.
Fernández-Friera L, Fuster V, López-Melgar B, et al. Normal LDL-cholesterol levels are associated with subclinical atherosclerosis in the absence of risk factors. J Am Coll Cardiol. 2017;70(24):2979-2991.
Gottlieb I, Miller JM, Arbab-Zadeh A, et al. The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol. 2010;55(7):627-634.
Valenti V, Ó Hartaigh B, Heo R, et al. A 15-year warranty period for asymptomatic individuals without coronary artery calcium: a prospective follow-up of 9,715 individuals. JACC Cardiovasc Imaging. 2015;8(8):900-909.
Budoff MJ, Young R, Lopez VA, et al. Progression of coronary calcium and incident coronary heart disease events: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2013;61(12):1231-1239.
Lehmann N, Erbel R, Mahabadi AA, et al. Value of progression of coronary artery calcification for risk prediction of coronary and cardiovascular events: result of the HNR study (Heinz Nixdorf Recall). Circulation. 2018;137(7):665-679.
Min JK, Lin FY, Gidseg DS, et al. Determinants of coronary calcium conversion among patients with a normal coronary calcium scan: what is the warranty period for remaining normal? J Am Coll Cardiol. 2010;55(11):1110-1117.
Bhanpuri NH, Hallberg SJ, Williams PT, et al. Cardiovascular disease risk factor responses to a type 2 diabetes care model including nutritional ketosis induced by sustained carbohydrate restriction at 1 year: an open label, non-randomized, controlled study. Cardiovasc Diabetol. 2018;17(1):56.
Yeboah J, McClelland RL, Polonsky TS, et al. Comparison of novel risk markers for improvement in cardiovascular risk assessment in intermediate-risk individuals. JAMA. 2012;308(8):788-795.
Dedic A, Lubbers MM, Schaap J, et al. Coronary CT angiography for suspected ACS in the era of high-sensitivity troponins: randomized multicenter study. J Am Coll Cardiol. 2016;67(1):16-26.
Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary. Circulation. 2019;139(25):e1046-e1081.
Mortensen MB, Falk E, Li D, et al. Statin trials, cardiovascular events, and coronary artery calcification: implications for a trial-based approach to statin therapy in MESA. JACC Cardiovasc Imaging. 2018;11(2 Pt 1):221-230.
Einstein AJ, Henzlova MJ, Rajagopalan S. Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007;298(3):317-323.
Interesting read thanks. Any comments on the below?
Zero Coronary Artery Calcium Score Desirable, but Enough? 2020
https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.119.045026
"About one-fourth to one-third of the total incident cardiovascular disease (CVD) events occur in those with a CAC of zero"