
The diet wars: what the science actually says
Reviewing the evidence every dietary tribe claims to have

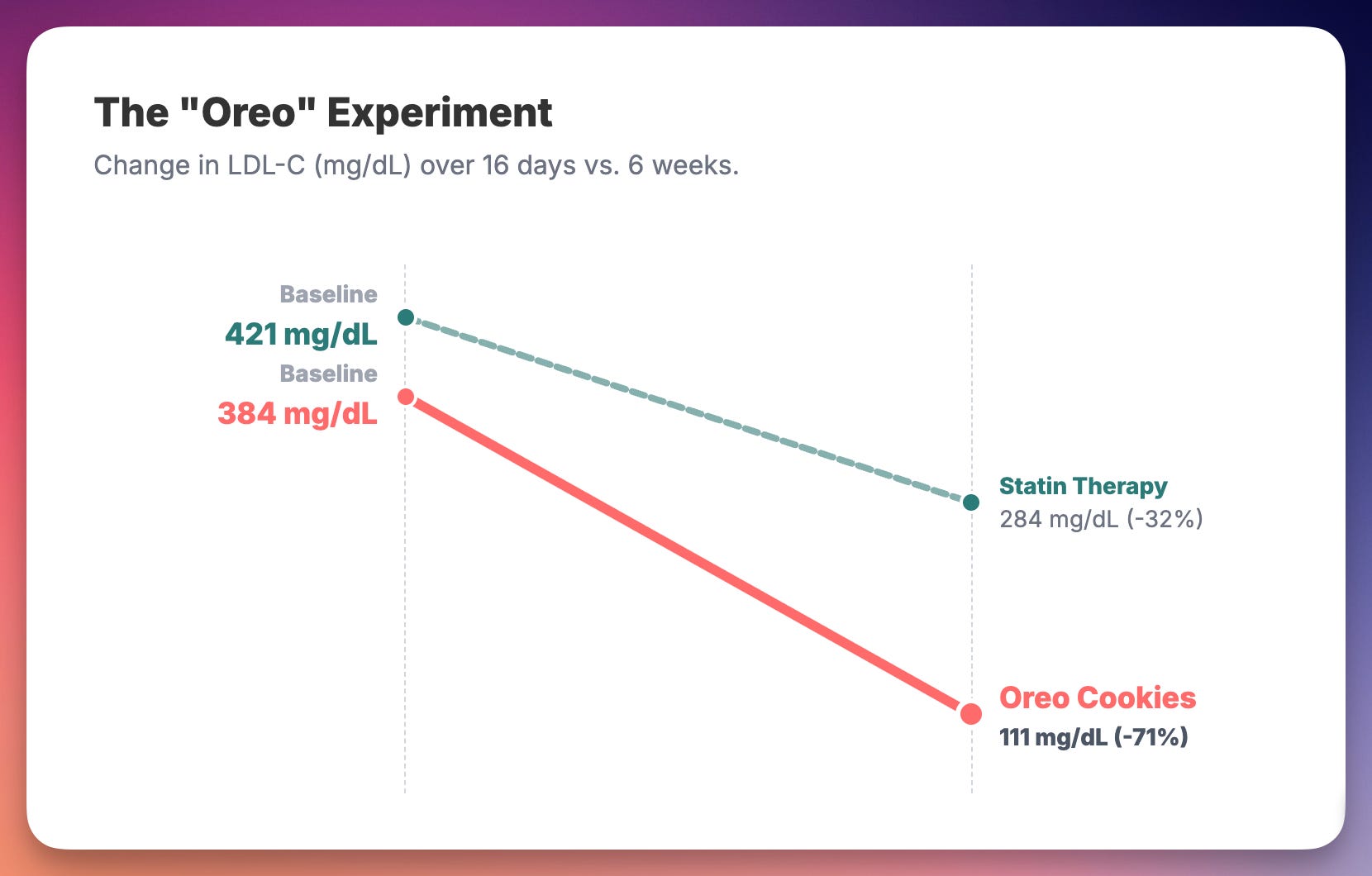
In 2024, a Harvard researcher published a case study showing that eating 12 Oreo cookies daily for 16 days lowered LDL cholesterol by 71%—while rosuvastatin 20mg achieved only 32.5%. The patient’s LDL dropped from 384 mg/dL to 111 mg/dL. The paper was peer-reviewed and published in Metabolites.(1)

If this sounds absurd, congratulations. You’ve just experienced what the diet wars feel like from the inside.
The study wasn’t a prank. It was designed to test the “Lipid Energy Model” in a specific phenotype called Lean Mass Hyper-Responders—metabolically healthy individuals whose LDL skyrockets on ketogenic diets. The Oreos weren’t magic. They provided 100 grams of carbohydrates that shifted the metabolic machinery away from fat oxidation. The point wasn’t that Oreos are healthy. The point was that context determines everything.
And yet, this single case study has been wielded by low-carb critics as evidence that keto is dangerous, and by keto advocates as evidence that LDL elevation on their diet is mechanistically distinct and therefore benign. Same data. Opposite conclusions. Welcome to the diet wars.
The tribal landscape
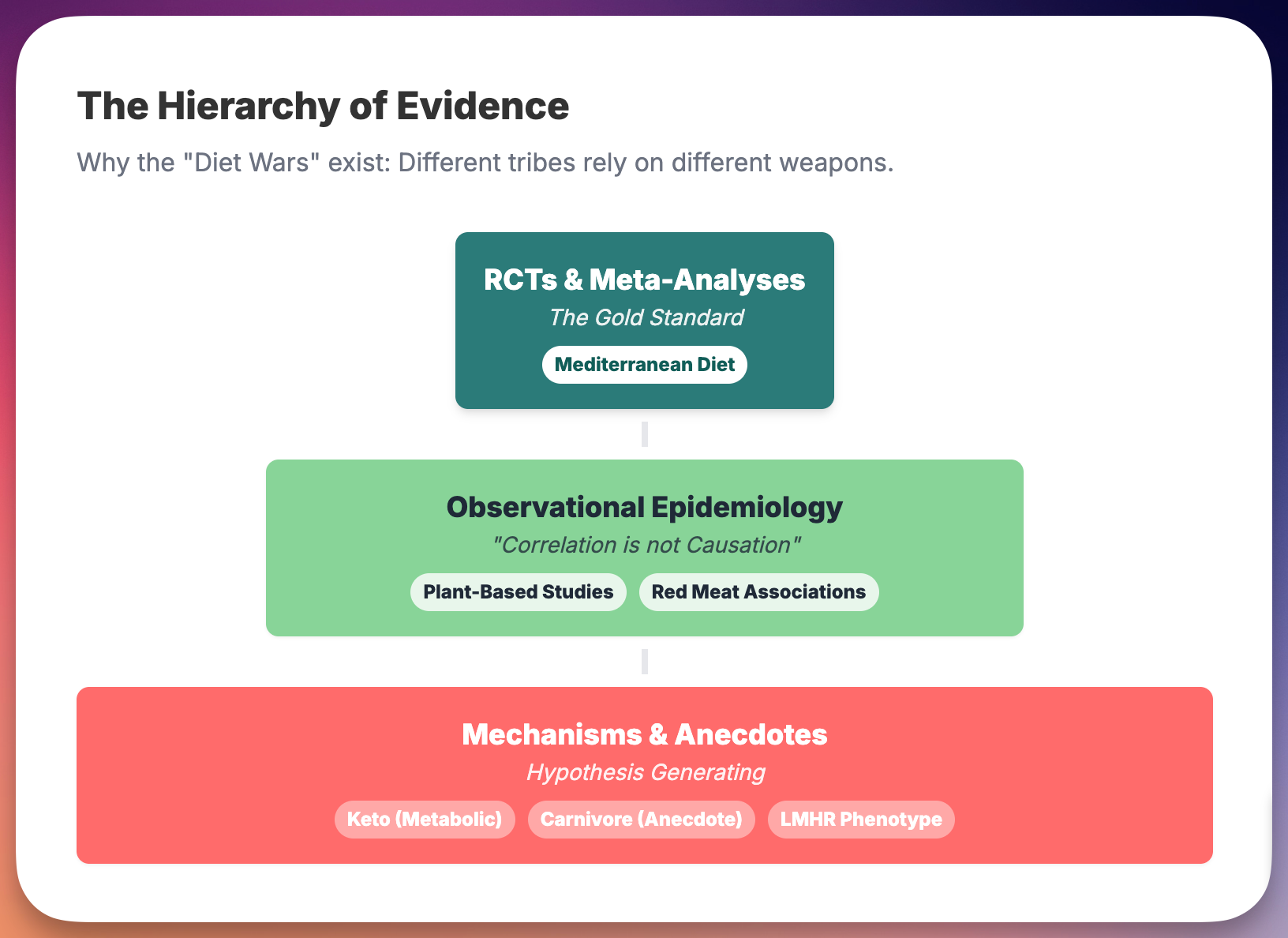
Vegans cite research showing plant-based diets reduce cardiovascular disease. Carnivores cite research showing red meat associations are weak and confounded. Keto enthusiasts cite diabetes reversal data. Mediterranean diet proponents cite the only large RCT with hard cardiovascular endpoints. Each tribe has PhDs, peer-reviewed papers, and passionate certainty.
The problem isn’t that any of them are lying. The problem is that nutrition science is genuinely difficult, and motivated reasoning is genuinely easy.
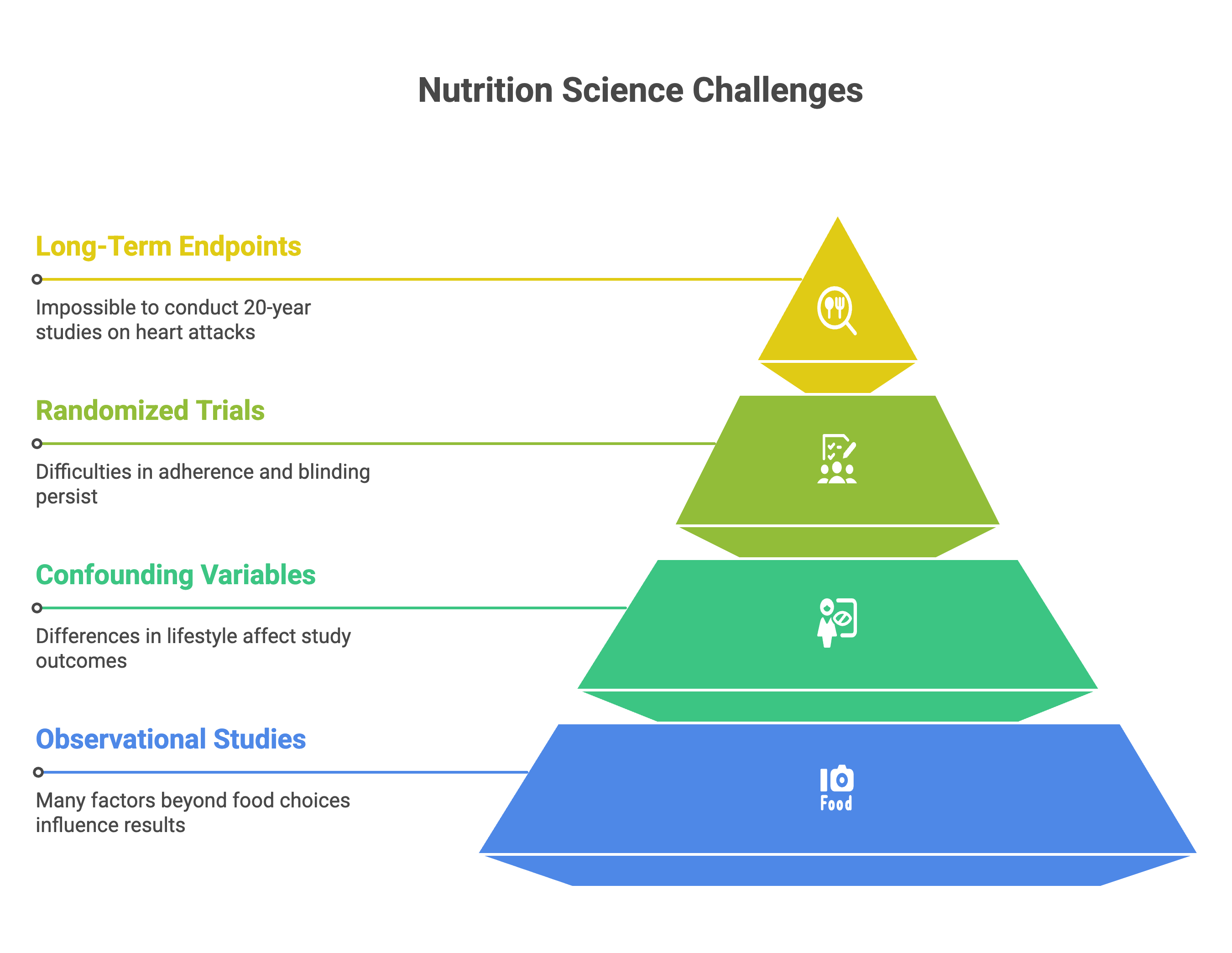
Most diet studies are observational. People who choose to eat plant-based differ from people who choose carnivore in dozens of ways beyond their food choices—exercise habits, smoking rates, socioeconomic status, health consciousness. Adjusting for confounders helps, but residual confounding persists. And even randomized trials struggle with adherence, blinding (you know if you’re eating steak or tofu), and the impossibility of running 20-year studies on hard endpoints like heart attacks and death.
So what do we actually know? Let me walk through the major diet camps and the highest-quality evidence for each.
The Mediterranean diet: the closest thing to a winner
If any dietary pattern has earned the right to claim cardiovascular benefit, it’s the Mediterranean diet. The PREDIMED trial randomized 7,447 high-risk Spanish adults to either a Mediterranean diet supplemented with extra-virgin olive oil, a Mediterranean diet supplemented with mixed nuts, or a control diet with advice to reduce fat. After a median follow-up of 4.8 years, both Mediterranean arms showed roughly 30% reduction in major adverse cardiovascular events compared to control.(2)
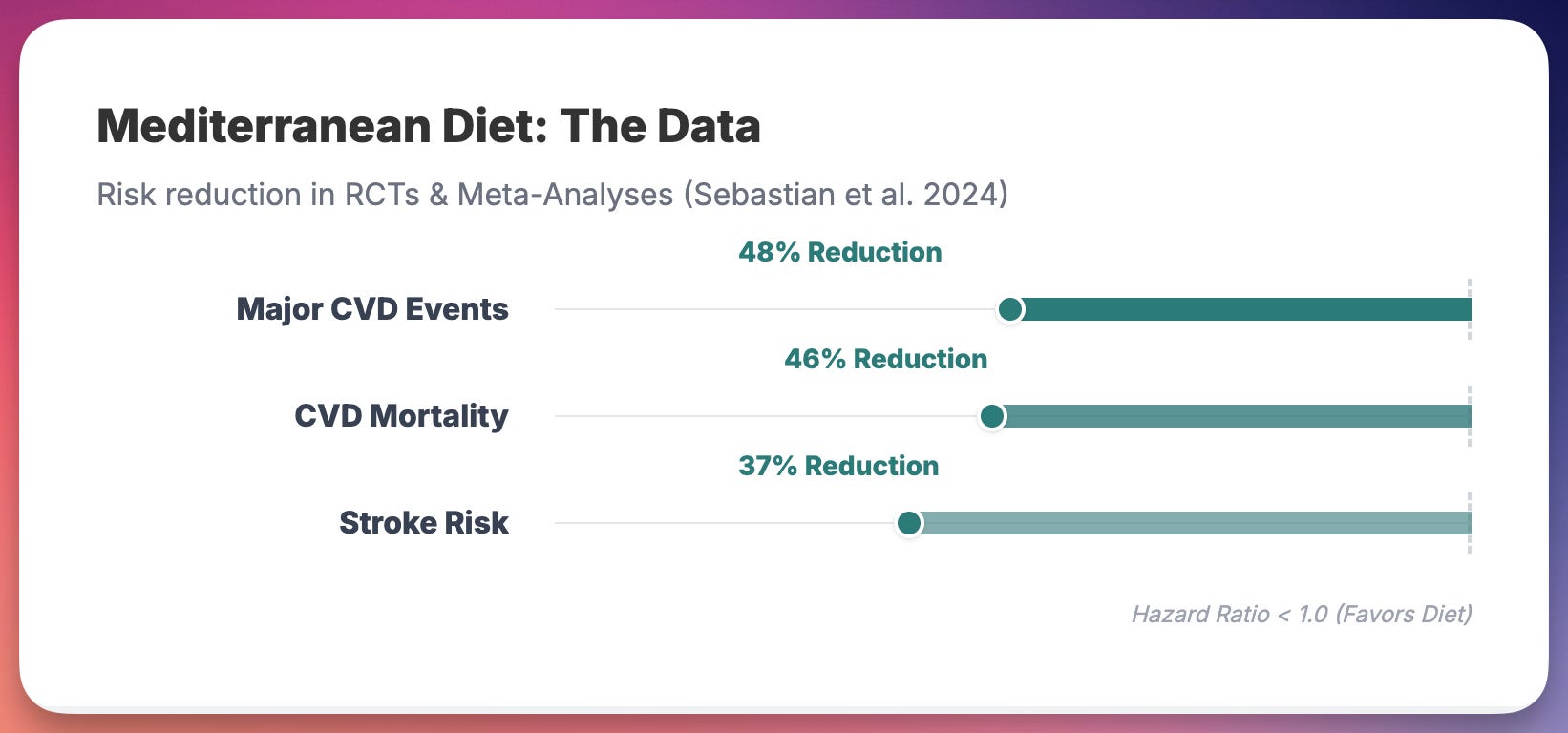
The trial was stopped early because the benefit was clear. A 2024 meta-analysis pooling PREDIMED with three other RCTs (Lyon Diet Heart Study, Indo-Mediterranean Diet Heart Study, CORDIOPREV) found that Mediterranean diet reduced the composite of MI, stroke, and cardiovascular death by 48% (OR 0.52, 95% CI 0.32-0.84) (3). Stroke risk dropped by 37%. Cardiovascular mortality dropped by 46%.
This is the gold standard. Randomized. Hard endpoints. Replicated across multiple trials. The Mediterranean diet is not a fad. It is the only dietary pattern with this level of evidence for cardiovascular protection.
Critics note that PREDIMED had some randomization irregularities in a subset of participants, leading to a retraction and republication with corrected analyses. The corrections didn’t meaningfully change the results. A comprehensive review in Circulation Research concluded that the criteria for causality were met and the evidence is “large, strong, and consistent” (4).
Plant-based diets: real benefits, real gaps
Vegetarian and vegan diets have accumulated substantial observational evidence. A 2022 meta-analysis of 13 cohort studies involving 844,175 participants found that vegetarians had 15% lower risk of cardiovascular disease (RR 0.85) and 21% lower risk of ischemic heart disease compared to non-vegetarians (5). The association with IHD was deemed “probably causal” using rigorous WCRF criteria.
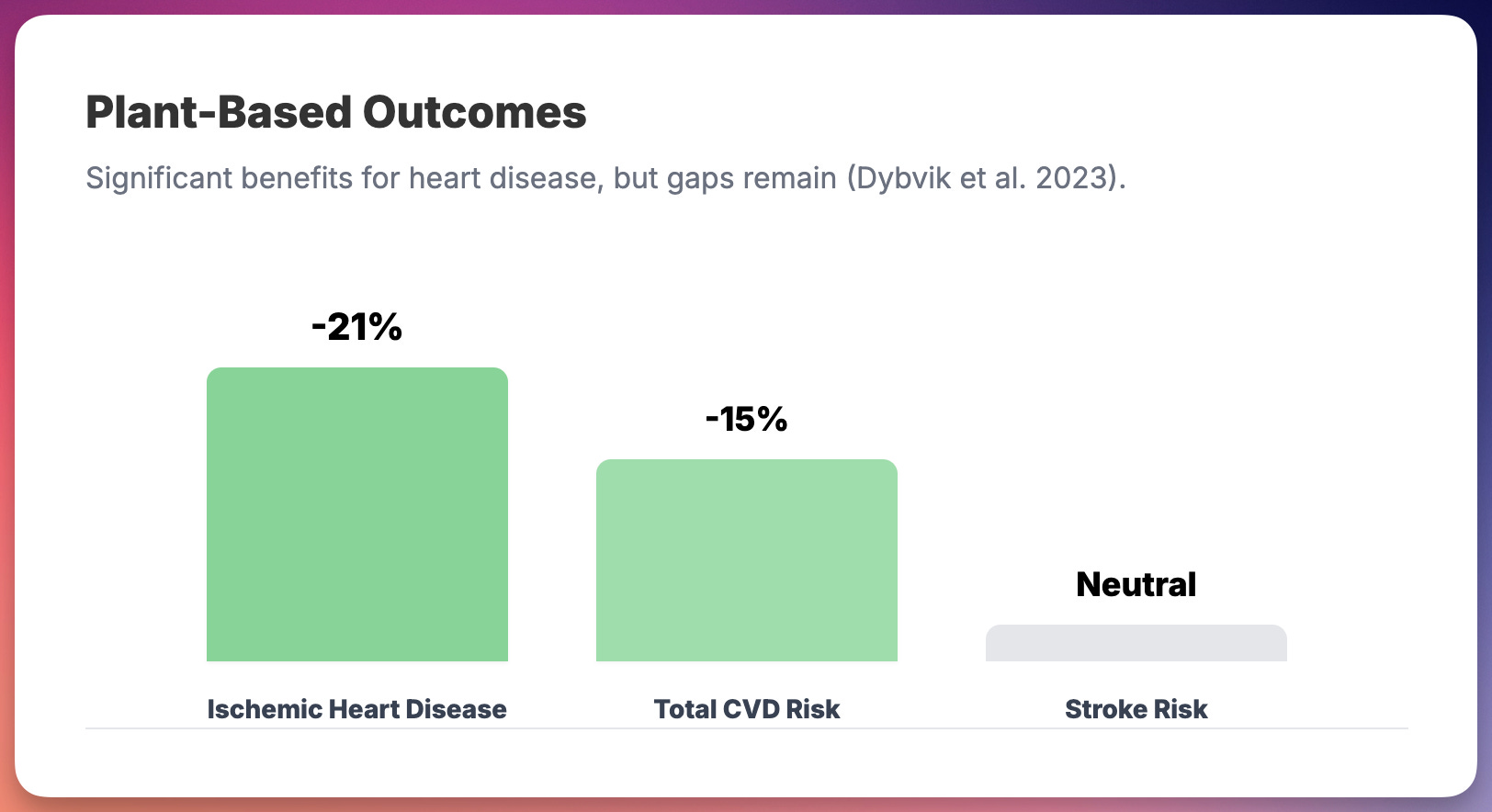
But there’s a catch. The same meta-analysis found no significant reduction in stroke risk among vegetarians. And a 2023 European Heart Journal review made a crucial distinction: not all plant-based foods are equally healthy (6). Diets rich in refined grains, sugary beverages, and processed vegetarian foods show increased mortality despite being technically “plant-based.” The quality of plant foods matters as much as the absence of animal foods.
I see B12 deficiency regularly in my practice. In India, where vegetarianism is culturally prevalent, this isn’t rare—it’s common. Prolonged deficiency causes irreversible neurological damage. Iron, zinc, and calcium deficiencies also occur with poorly planned vegetarian diets. These aren’t theoretical concerns. They’re clinical realities that don’t make it into the advocacy literature.
The evidence supports well-planned plant-based diets for cardiovascular risk reduction. It does not support the claim that eliminating all animal products is necessary or universally optimal.
The ketogenic diet: metabolic benefits, lipid concerns
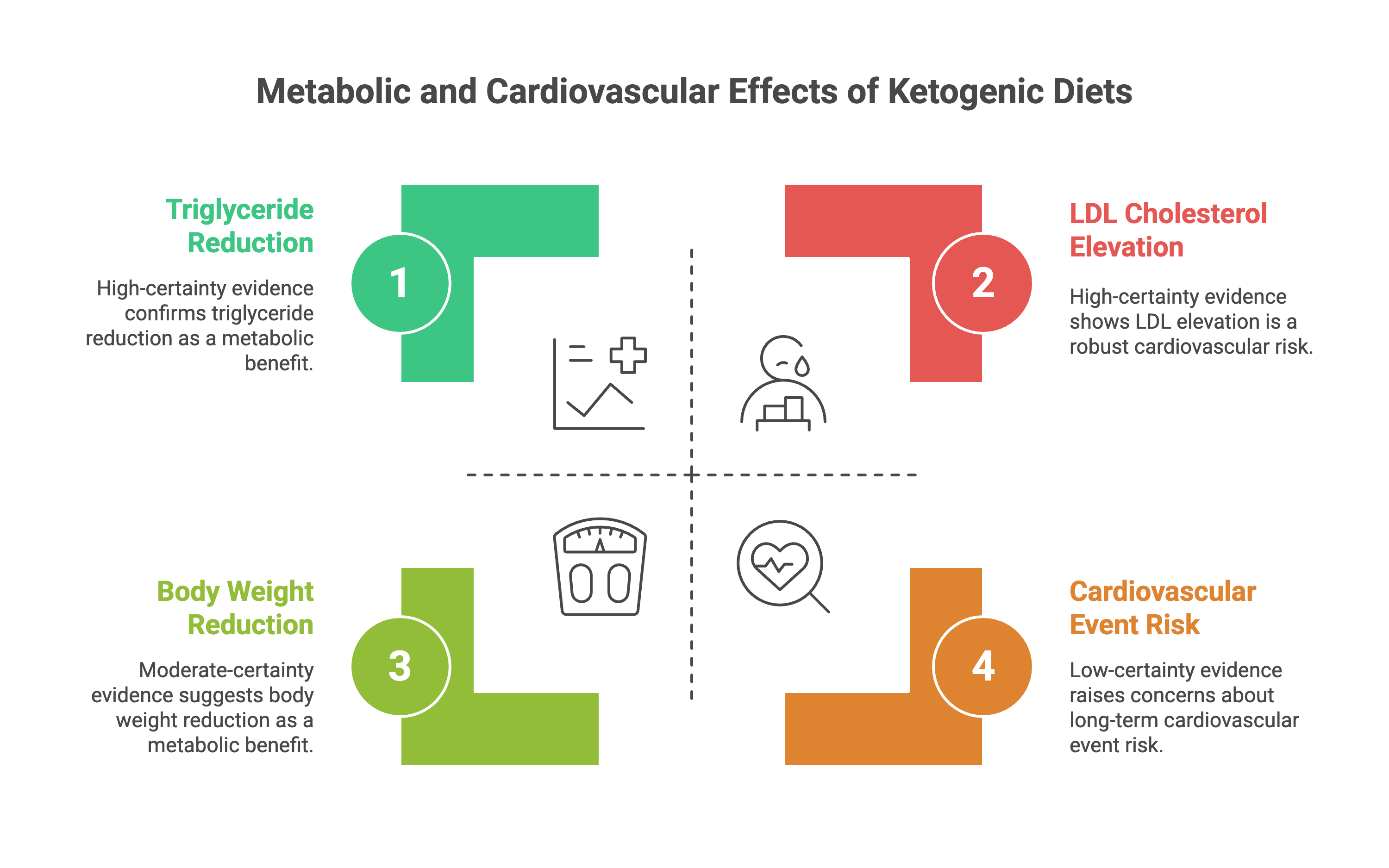
Ketogenic diets produce rapid, measurable improvements in several metabolic markers. A 2023 umbrella review in BMC Medicine synthesized 17 meta-analyses covering 68 randomized trials (7). The findings were telling.
High-certainty evidence showed that ketogenic diets reduce triglycerides and reduce seizure frequency in epilepsy. Moderate-certainty evidence showed reductions in body weight, HbA1c, and respiratory exchange ratio. For weight loss and glycemic control, particularly in type 2 diabetes, the short-term data are favorable.
But the same umbrella review found high-certainty evidence that ketogenic diets increase LDL cholesterol. This is not a minor footnote. LDL elevation is the most robustly established causal risk factor for atherosclerotic cardiovascular disease. The authors concluded: “Clinical trials with long-term follow-up are warranted to investigate whether the short-term effects of KD will translate to beneficial effects on clinical outcomes such as cardiovascular events and mortality.”
We don’t have those trials. The keto community often dismisses LDL concerns by pointing to improvements in triglycerides and HDL. But the ratio doesn’t override the absolute LDL risk in populations with established cardiovascular disease. In my practice, I’ve seen patients on ketogenic diets with LDL levels exceeding 300-400 mg/dL. These are not numbers I can ignore, regardless of how good their triglyceride-to-HDL ratio looks.
The lean mass hyper-responder puzzle
The most intellectually honest keto advocates acknowledge the LDL problem and point to emerging research on Lean Mass Hyper-Responders. These are metabolically healthy, often lean individuals whose LDL rises dramatically on carbohydrate restriction—sometimes exceeding 500 mg/dL—while maintaining very high HDL and very low triglycerides.
The KETO-CTA trial, published in JACC Advances in 2024, compared 80 such individuals (mean LDL 272 mg/dL, some as high as 591 mg/dL) to matched controls with average LDL of 123 mg/dL (8). Using coronary CT angiography, the researchers found no significant difference in plaque burden between groups. No correlation between LDL level and plaque. In a 2025 follow-up with longitudinal imaging, they reported that baseline plaque predicted plaque progression, but ApoB and LDL exposure did not (9).
This is genuinely surprising and deserves attention. But context matters. The mean duration on ketogenic diet was 4.7 years. Atherosclerosis develops over decades. The sample was 80 people—highly selected, metabolically exceptional individuals. And coronary plaque on CT is a surrogate marker, not a hard clinical endpoint. We don’t know if these individuals will have more heart attacks in 20 years.
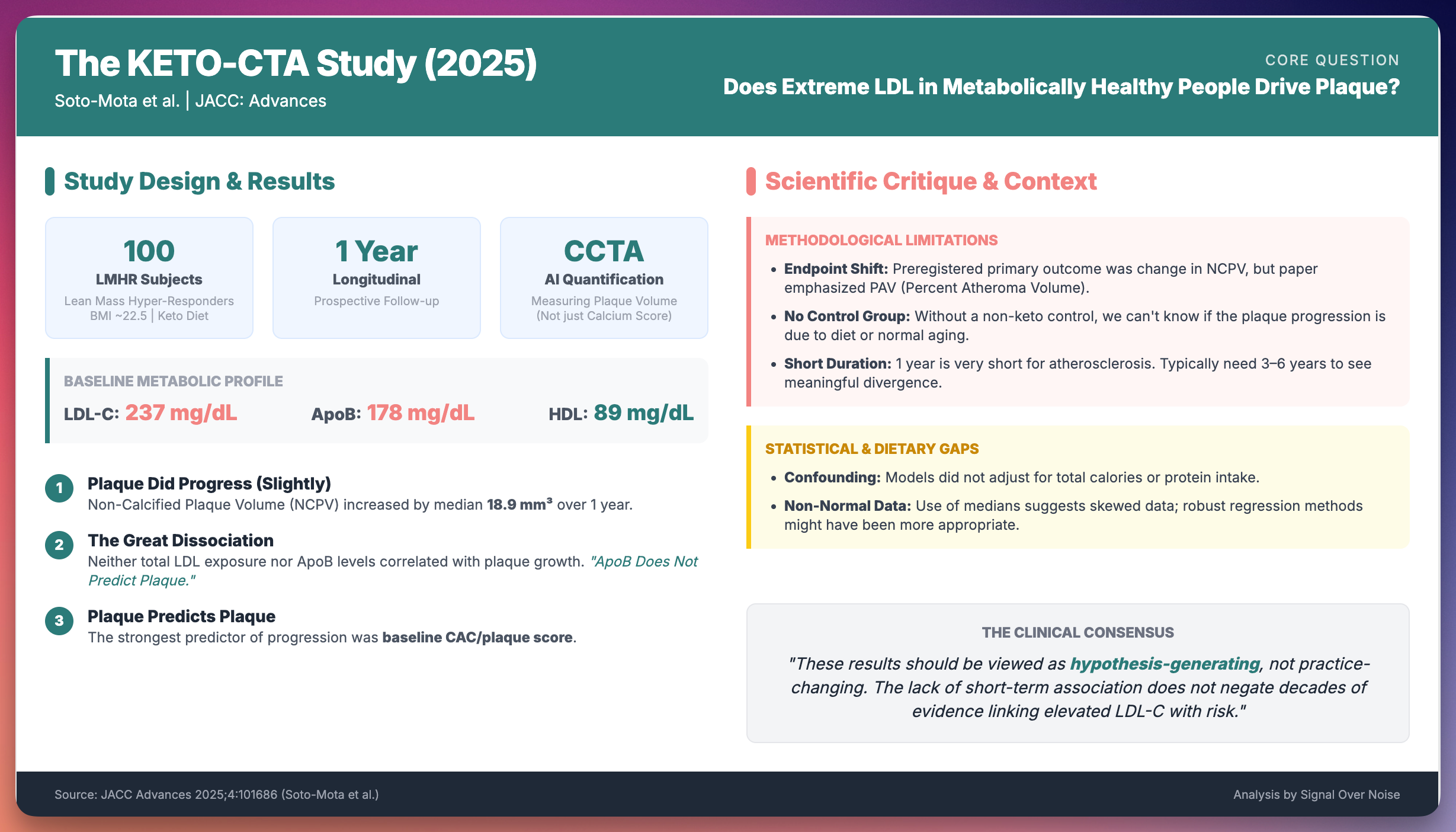
The LMHR data is hypothesis-generating. It suggests that the relationship between LDL and cardiovascular risk may be context-dependent in ways we don’t fully understand. It does not prove that sky-high LDL is safe in any population. The authors themselves emphasized that their findings “should provoke further research and not be seen as health advice.”
Red meat and the carnivore question
The carnivore diet—eating exclusively animal products—has no randomized trial data on cardiovascular outcomes. Its proponents rely primarily on critiques of observational studies linking red meat to disease.
Those critiques aren’t baseless. A 2019 systematic review in Annals of Internal Medicine analyzed 61 articles from 55 cohorts with over 4 million participants (10). The authors concluded that the association between red and processed meat consumption and adverse cardiometabolic outcomes is “very small” and the evidence is “of low certainty.” This paper generated enormous controversy precisely because it challenged dietary guidelines that many considered settled.
A 2020 JAMA Internal Medicine study of 29,682 US adults found that each additional 2 servings per week of unprocessed red meat was associated with a 3% increased risk of incident cardiovascular disease (11). Statistically significant, but the absolute risk increase was small—about 0.6% over 30 years. Processed meat showed slightly stronger associations.
The honest summary: observational data consistently show small associations between red meat intake and cardiovascular risk. The magnitude is modest. The certainty is low. Confounding is substantial. We have no RCT evidence on carnivore diets and hard endpoints, and we’re unlikely to get any.
Absence of evidence is not evidence of safety. Advocates who claim carnivore diets are optimal for cardiovascular health are extrapolating far beyond what the data support.
What actually matters
After reviewing the highest-quality evidence from tier-1 journals, a few conclusions survive the tribal warfare.
First, dietary patterns matter more than single nutrients or foods. The Mediterranean diet’s benefit likely comes from the overall pattern—olive oil, nuts, fish, vegetables, legumes, moderate wine—not from any single component. Obsessing over whether eggs raise cholesterol or whether saturated fat is “actually fine” misses the forest for the trees.
Second, ultra-processed foods are probably the real enemy. Across dietary ideologies, from plant-based to paleo, the consistent signal is that whole, minimally processed foods outperform their industrial counterparts. An unhealthy vegetarian diet heavy in refined carbs and processed meat alternatives increases mortality. A keto diet built on processed cheese and bacon is not the same as one built on fish, avocado, and olive oil.
Third, individual variation is real but poorly understood. The LMHR phenotype demonstrates that the same diet produces different metabolic responses in different people. We’re only beginning to understand why. Precision nutrition remains more promise than reality, but it’s not wrong to acknowledge that dietary recommendations may need individualization.
Fourth, long-term data on hard endpoints remain scarce for most diets. The Mediterranean diet has it. Plant-based diets have supportive observational data. Ketogenic and carnivore diets have metabolic studies and surrogate markers. Anyone claiming certainty about 20-year cardiovascular outcomes from these latter diets is overstating the evidence.
The boring truth
The diet wars persist because uncertainty is uncomfortable and tribal identity is appealing. It’s more satisfying to believe you’ve found the One True Diet than to acknowledge that nutrition science is messy, context-dependent, and evolving.
The Oreo study that opened this piece wasn’t evidence that cookies are healthy. It was a mechanistic demonstration in a single unusual patient. But it became a weapon in tribal combat within hours of publication. That’s how the diet wars work. Data becomes ammunition. Context becomes collateral damage.
As a cardiologist, my job isn’t to pick a dietary tribe. It’s to read the evidence carefully, acknowledge uncertainty honestly, and help patients make decisions that fit their metabolic reality, their preferences, and their risk profile. For most people, that means something closer to Mediterranean than to any extreme—more plants, more olive oil, more fish, fewer processed foods, and less obsession with dietary purity.
The science isn’t as exciting as the wars. But it’s more useful.
If you found this analysis valuable, please share it.
Evidence over opinions. Clarity over noise. That’s Signal Over Noise.
Thanks - a nice summary. Any comments on this recent paper? Matches the Mediterranean story pretty much
100,000+ people followed for 30 years
* 9% had 0 of 11 chronic diseases tracked
* The same 9% had no cognitive, physical or mental impairments by age 70
Mostly plants, some animal i.e. Mediterranean
Optimal dietary patterns for healthy aging, 2025
https://www.nature.com/articles/s41591-025-03570-5