
Statins & Brain Fog : What's Really Happening to Your Brain on Statins?
Will my statin make me forget things?

You have been started on a statin for whatever reason and now you are on X or social media and now you’ve worried about your memory, you’re not alone. When I talk about statins on social media, nearly half of the people bring up concerns about their brain. “I’ve been foggy since I started this medication.” “I can’t find words like I used to.” “My friend says statins cause dementia.”

These concerns are real, and they deserve a real answer, not a dismissive “don’t worry about it” or a complicated lecture about clinical trials. So let me walk you through what we actually know, what we don’t know, and what it means for you.
Where does this fear come from?
In 2012, the FDA added a warning to statin labels about potential memory problems. This made headlines. Patients got scared. Doctors got questions. And a lot of people stopped taking their statins.

But here’s what most news stories didn’t explain: the FDA based this warning on reports that patients and doctors voluntarily submitted - not on controlled studies designed to test whether statins actually affect memory. When someone reports a side effect while taking a medication, that doesn’t prove the medication caused it. It just means the two things happened around the same time.
Think of it this way: millions of people start statins in their 50s and 60s. That’s also the age when memory naturally starts to change for everyone—statin or no statin. If you happen to notice your memory slipping after starting a statin, it’s natural to connect the two. But that connection might be coincidence, not cause.
So researchers set out to test this properly.
What happens when you actually test this carefully?
The gold standard in medicine is called a randomized controlled trial. You take a large group of people, randomly assign half to get the real medication and half to get a placebo (a dummy pill), and then compare what happens—without anyone knowing which pill they got. This removes the bias of expectation.
When researchers combined the results of 25 such trials involving nearly 47,000 people, they found something clear: people taking statins performed exactly the same on memory and thinking tests as people taking placebo pills. No difference. Not even a small trend toward harm. This held true whether people had normal memory to begin with or already had Alzheimer’s disease. (Ott et al., 2015)
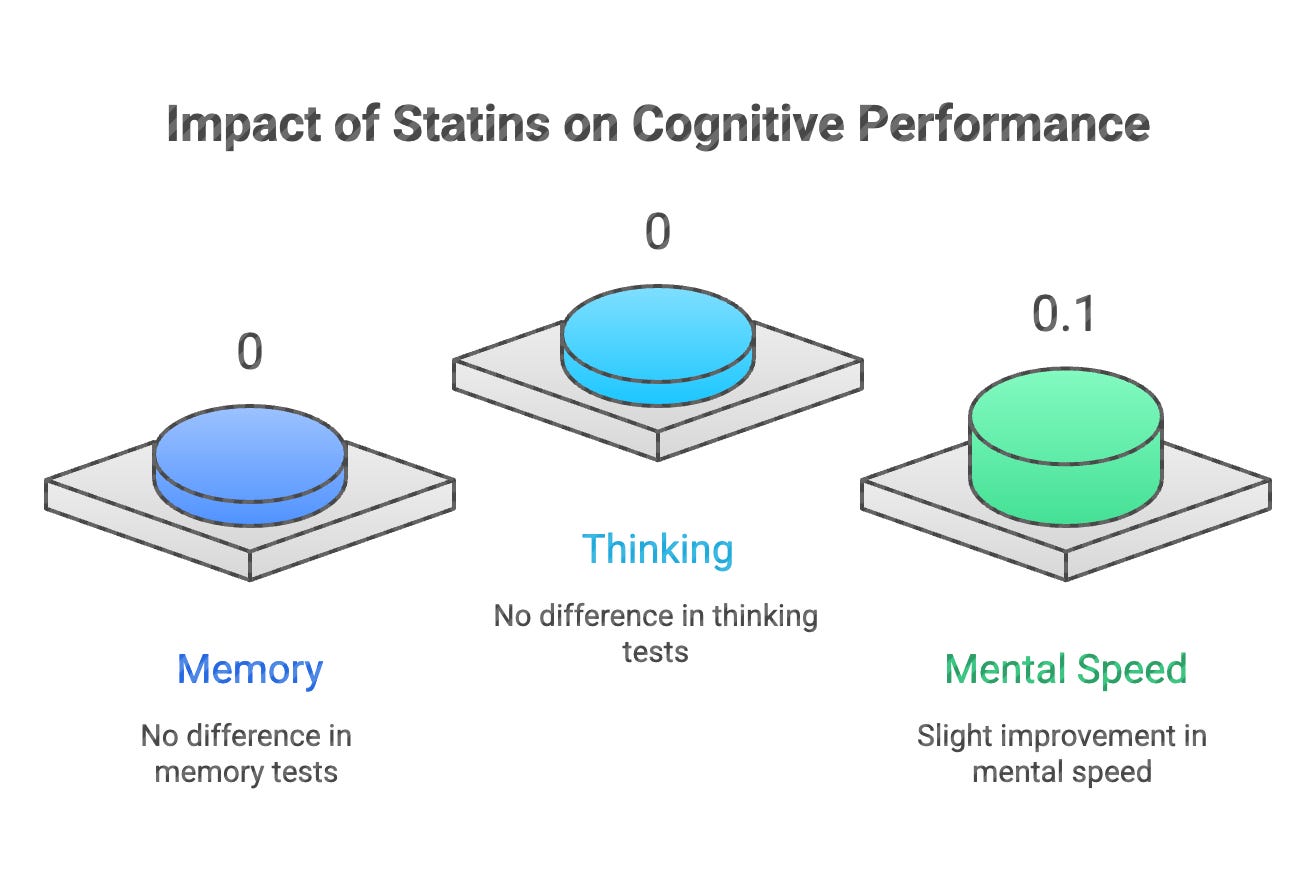
A larger analysis looked at 33 studies with over 128,000 people. Same finding. Despite dramatically lowering cholesterol, statins didn’t change rates of memory problems or dementia. The only measurable difference? People on statins actually performed slightly better on tests of mental speed. (Ying et al., 2020)
These aren’t small studies done by drug companies. These are independent researchers combining decades of data, looking specifically for harm - and not finding it.
So why do so many people feel foggy on statins?
This is where it gets interesting and it involves something called the nocebo effect.
You’ve probably heard of the placebo effect: give someone a sugar pill but tell them it’s pain medication, and some of them will actually feel less pain. Their expectation creates a real physical experience.
The nocebo effect is the opposite. Tell someone a medication might cause headaches, and some of them will get headaches—even if they’re taking a sugar pill.
A remarkable study demonstrated this with statins. Researchers in the UK followed over 10,000 people, first in a phase where neither patients nor doctors knew who was getting atorvastatin versus placebo, and then in a phase where everyone knew.
During the blinded phase, when nobody knew who was on the real drug, muscle complaints were identical in both groups ~ 2% per year. Cognitive problems were too rare to even measure meaningfully.
But during the unblinded phase, when people knew they were taking a statin, muscle complaints suddenly jumped 41% higher in the statin group. The medication hadn’t changed. Only awareness of taking it had changed. (Gupta et al., Lancet 2017)
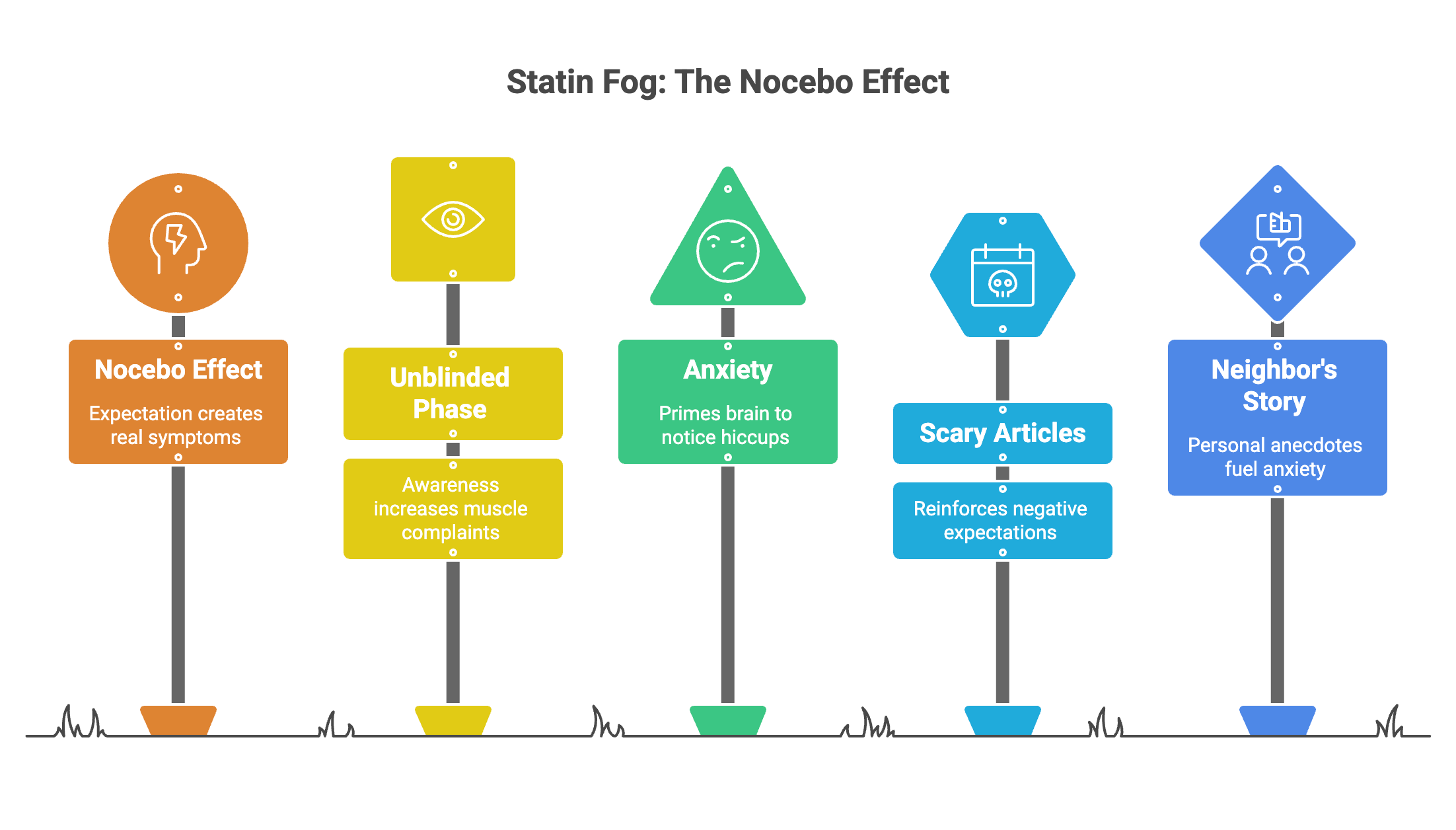
This doesn’t mean people are making up their symptoms. Nocebo effects are real experiences in your body: real pain, real fog, real fatigue. But they’re generated by expectation and anxiety rather than by the chemistry of the drug itself.
When you’ve read scary articles about statins and memory, when your neighbor told you her husband “was never the same” after starting one, when you’re already worried about getting older, your brain is primed to notice and attribute any mental hiccup to the pill.
Can statins actually protect the brain?
Here’s something that might surprise you: if anything, the evidence leans toward statins being good for your brain, not bad.
This makes sense when you think about what statins do. They lower cholesterol, yes, but they also reduce inflammation and improve blood vessel health throughout your body—including the blood vessels feeding your brain. Many types of dementia, including some cases of Alzheimer’s, involve problems with blood flow to the brain. A medication that keeps blood vessels healthy might protect against this.
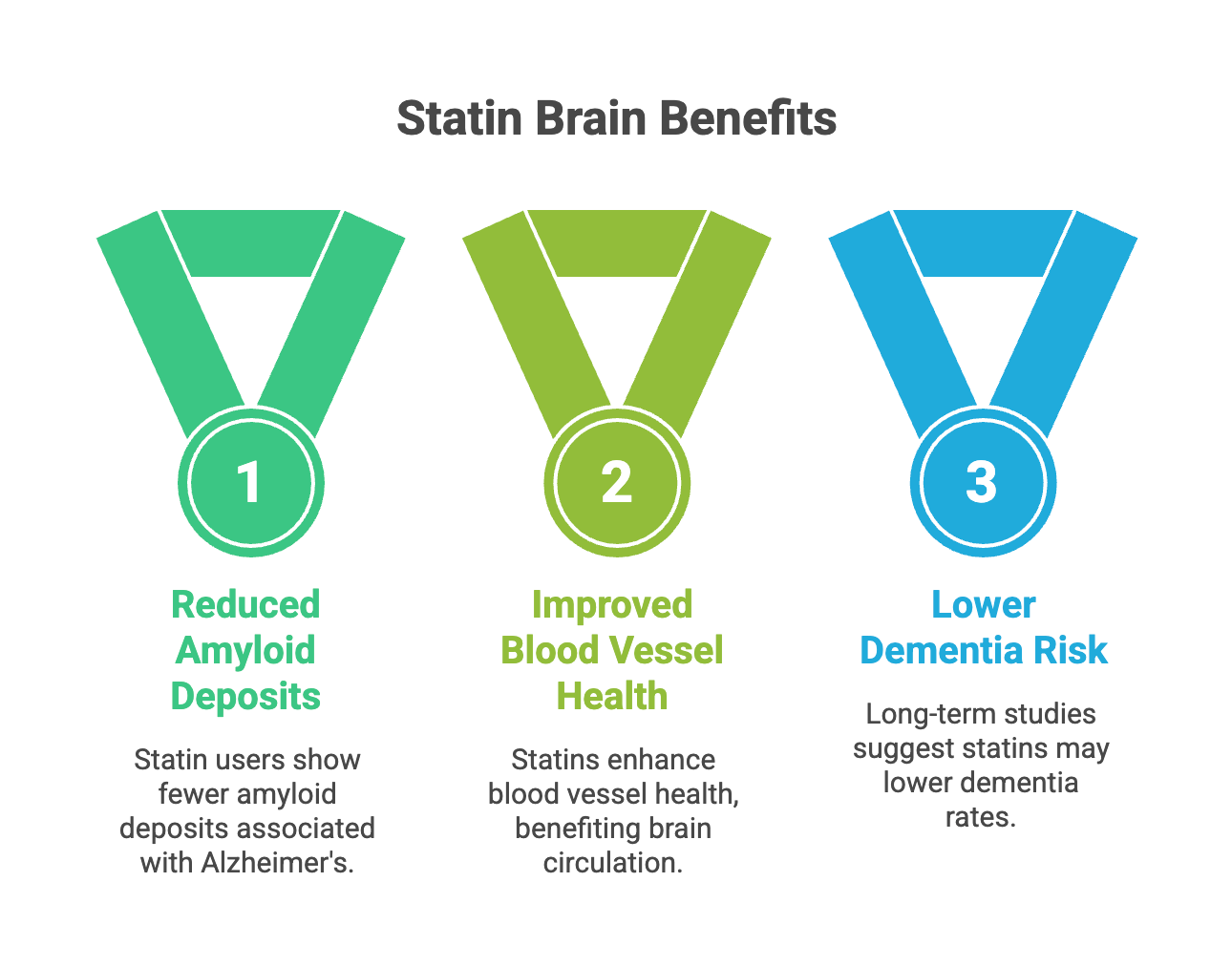
Long-term studies following older adults for up to 12 years found that statin users were actually less likely to have the protein deposits (called amyloid) associated with Alzheimer’s disease. Statin use wasn’t associated with faster memory decline or higher dementia rates. (Arvanitakis et al., 2008)
Now, this doesn’t prove statins prevent Alzheimer’s. These were observational studies, meaning we’re watching what happens to people who chose to take statins versus those who didn’t, and those groups might differ in other ways. But it’s reassuring that after following tens of thousands of people for years, researchers keep finding either no effect or a slight benefit, never clear harm.
What about people who already have memory problems?
Researchers also tested whether giving statins to people with diagnosed Alzheimer’s disease would help or hurt.
In the largest such trial, 640 patients with mild to moderate Alzheimer’s took either high-dose atorvastatin or placebo for 72 weeks while continuing their other Alzheimer’s medications. The result? No difference. The statin didn’t help their memory, but it didn’t hurt it either. (Feldman et al., Neurology 2010)
This fits a pattern: statins seem neutral for the brain. They don’t appear to accelerate decline, but they don’t reverse existing damage either. Their potential value is probably in prevention—keeping blood vessels healthy over decades—rather than treatment once problems have started.
The brain makes its own cholesterol
One reason people worry about statins and the brain involves a misunderstanding about cholesterol.
Your brain contains about 25% of your body’s total cholesterol, even though it’s only 2% of your body weight. Cholesterol is essential for brain cells to function—it’s part of every cell membrane and helps nerve signals travel.
But here’s the key point most people don’t know: your brain makes its own cholesterol. The cholesterol in your blood can’t cross into your brain. There’s a barrier—the blood-brain barrier—that prevents this. So the cholesterol your statin is lowering in your bloodstream isn’t the same pool of cholesterol your brain uses.
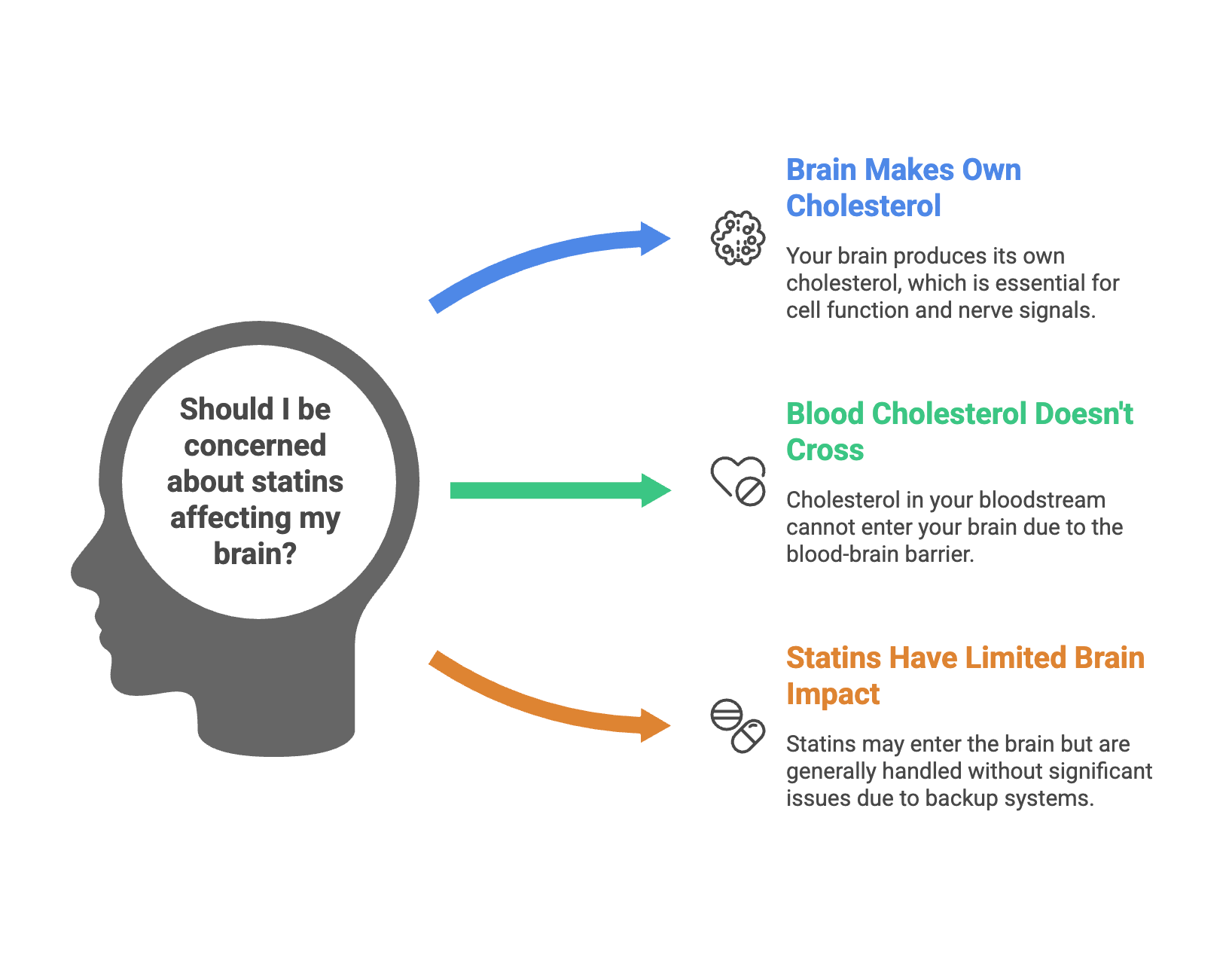
Statins do get into the brain to some degree and can affect cholesterol production there. But the brain has backup systems and tightly regulates its own cholesterol supply. In most people, this system handles statin exposure without any problem. (Allen et al., 2019)
Could some people genuinely be more sensitive?
Honesty requires acknowledging what we don’t fully understand.
Most people tolerate statins without any effect on their thinking. The large trials prove this at the population level. But medicine treats individuals, not populations, and some individuals do report real improvement when they stop their statin. What might explain this?
One clue comes from the differences between statins themselves. Statins aren’t all identical. Some like simvastatin and atorvastatin—dissolve easily in fat, which means they can slip into the brain more readily. Others like pravastatin and rosuvastatin—dissolve in water and have a harder time crossing from blood into brain tissue. A review examining all available evidence found that the rare reports of cognitive trouble came mostly from the fat-soluble statins, not the water-soluble ones. (Rojas-Fernandez et al., 2012)
This makes biological sense. Your brain makes its own cholesterol and tightly controls its supply. A statin that can’t easily get into the brain won’t affect this process. A statin that penetrates more deeply might—in some people—temporarily interfere with the brain’s cholesterol production.
Research in mice helps explain what might happen in that sensitive minority. When researchers gave mice simvastatin (a fat-soluble statin) for extended periods, they found the drug did reduce cholesterol levels in the hippocampus—the brain region crucial for memory—and the mice performed worse on memory tasks. But here’s the important part: when they stopped the drug, the brain’s cholesterol levels returned to normal, the connections between brain cells recovered, and the memory problems disappeared. (Guo et al., 2021)
This reversibility is reassuring. Even in an animal model specifically designed to show statin effects on the brain, the changes weren’t permanent. Stop the drug, and the brain bounces back.
What does this mean practically? If you’re one of the rare individuals who genuinely experiences cognitive changes on a statin, you have options beyond simply stopping all cholesterol treatment:
You can try a different statin. Switching from a fat-soluble statin like simvastatin or atorvastatin to a water-soluble one like pravastatin or rosuvastatin might eliminate the problem while still protecting your heart. Several clinical reports suggest this works. (Rojas-Fernandez et al., 2012)
You can use a lower dose. The degree to which any statin affects the brain likely depends on how much reaches brain tissue—which depends partly on blood levels. Lower doses mean less drug available to cross into the brain.
You can add or switch to non-statin alternatives. Medications like ezetimibe block cholesterol absorption from your gut—they never even reach your brain. PCSK9 inhibitors work in your liver and don’t cross into the brain either. Combining a low-dose statin with these alternatives can achieve the same cholesterol-lowering while minimizing brain exposure.
The bottom line: even if you’re among the small minority who might be sensitive to statin effects on the brain, this isn’t a binary choice between protecting your heart and protecting your memory. The medical toolkit has expanded. And importantly, the evidence suggests that any cognitive effects from statins are reversible—your brain isn’t being permanently changed.
What if you’re convinced your statin is affecting your memory?
Take your concern seriously, but approach it carefully.
First, consider timing. Did your symptoms truly start with the statin, or were you already noticing changes that you’ve now attributed to the medication? Memory changes are common in middle age regardless of medication.
Second, consider the nocebo effect. If you’ve been anxious about statins, that anxiety itself can cause fatigue, difficulty concentrating, and mental fog. Anxiety is exhausting, and exhaustion makes thinking harder.
Third, talk to your doctor about a trial off the medication. This means stopping the statin for a defined period (usually a few weeks to a couple months) to see if your symptoms genuinely improve. If they do, you might try restarting to see if they return. If symptoms improve off the statin and worsen when you restart it, that’s meaningful information—even if it contradicts the population data.
Fourth, remember that alternatives exist. If you and your doctor conclude that you truly can’t tolerate a statin, other medications can lower cholesterol without affecting cholesterol production: ezetimibe blocks cholesterol absorption from food; PCSK9 inhibitors help your liver clear cholesterol from blood; bempedoic acid works earlier in the pathway than statins. You don’t have to choose between your brain and your heart.
The honest answer
Here’s what I’d tell my own family member asking this question:
The fear that statins cause memory problems is understandable but not supported by the evidence. When scientists have tested this carefully in tens of thousands of people, they’ve found no harm. Many people who believe their statin is causing brain fog are likely experiencing the nocebo effect—real symptoms caused by expectation and worry rather than by the drug’s chemistry.
At the same time, if you have persistent, bothersome cognitive symptoms that you strongly associate with your statin, it’s reasonable to discuss a trial discontinuation with your doctor. You’re not crazy. Your experience matters. But go into that conversation knowing that the odds favor a cause other than the statin.
For most people, statins remain among the most proven, safest, most effective medications we have for preventing heart attacks and strokes. The risk of stopping them is real and measurable. The risk of cognitive harm is theoretical and undetectable in large studies.
What we still don’t know
I want to be honest about the limits of our knowledge.
Until recently, no trial was specifically designed to answer the dementia question as its main purpose. The older trials looked at heart disease first and cognition second. But researchers recognized this gap—two major trials—STAREE (Zoungas et al., 2024) in Australia and PREVENTABLE (Joseph et al., 2023) in the United States—have enrolled nearly 30,000 older adults specifically to answer whether statins affect dementia risk.
We also don’t know whether starting a statin in your 40s versus your 70s makes a difference for brain health. We don’t know whether certain statins are better or worse for the brain than others. We don’t know whether people with certain genetic profiles respond differently.
These gaps should be filled with research, not fear. In the meantime, the preponderance of evidence says statins are safe for your brain—and the evidence of their heart benefits is overwhelming.
Thanks for reading and subscribing to Signal Over Noise.
If you found this helpful, please share it with anyone who’s worried about this question. Getting accurate information out matters—and it might help someone avoid stopping a medication that’s protecting their heart.
All content on Signal Over Noise is free and open-access.
References
Ott BR, et al. Do statins impair cognition? A systematic review and meta-analysis of randomized controlled trials. J Gen Intern Med. 2015;30(3):348-58.
Ying H, et al. Association of Statin Use With Risk of Dementia and Mild Cognitive Impairment. JAMA Network Open. 2020.
Gupta A, et al. Adverse events associated with unblinded, but not with blinded, statin therapy in the ASCOT-LLA trial. Lancet. 2017;389(10088):2473-2481.
Ruscica M, et al. Side effects of statins: from pathophysiology and epidemiology to diagnostic and therapeutic implications. Cardiovasc Res. 2023;118(17):3288-3304.
Feldman HH, et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology. 2010;74(12):956-64.
Arvanitakis Z, et al. Statins, incident Alzheimer disease, change in cognitive function, and neuropathology. Neurology. 2008;70(19):1795-802.
Allen LB, et al. Desmosterol and Desmosterolosis. Prostaglandins Leukot Essent Fatty Acids. 2019;143:1-4.
Bai X, et al. The role of DHCR24 in the pathogenesis of AD: re-cognition of the relationship between cholesterol and AD pathogenesis. Acta Neuropathol Commun. 2022;10(1):35.
Power MC, et al. Statins, cognition, and dementia—systematic review and methodological commentary. Nat Rev Neurol. 2015;11(4):220-9.
Wagstaff LR, et al. Statin-associated memory loss: analysis of 60 case reports and review of the literature. Pharmacotherapy. 2003;23(7):871-80.
Moon JY, et al. Characteristics of Subjective and Objective Statin-Related Adverse Events. Clin Pharmacol Ther. 2020;107(3):630-637.
Bitzur R. Remembering Statins: Do Statins Have Adverse Cognitive Effects? Diabetes Care. 2016;39 Suppl 2:S253-9.
Zoungas S. STAREE investigator group. Baseline Characteristics of Participants in STAREE: A Randomized Trial for Primary Prevention of Cardiovascular Disease Events and Prolongation of Disability-Free Survival in Older People. J Am Heart Assoc. 2024 Nov 19;13(22):e036357. doi: 10.1161/JAHA.124.036357. Epub 2024 Nov 15.
Joseph J. Pragmatic evaluation of events and benefits of lipid lowering in older adults (PREVENTABLE): Trial design and rationale. J Am Geriatr Soc. 2023 Jun;71(6):1701-1713. doi: 10.1111/jgs.18312. Epub 2023 Apr 20.
https://agsjournals.onlinelibrary.wiley.com/doi/10.1111/jgs.18312
Great work Dr. Shailesh. Been following you from Twitter. It's frustrating to see MANY doctors, even SPECIALISTS, don't have knowledge or curiosity or humility to consider alternate view points and be updated. I had a cardiologist at a reputed hospital tell me he doesn't believe in ctca or apob 😂. (not using is totally fair if pragmatic, not believing is arrogance in face of scientific evidence imho). This also puts us in a dangerous situation where effective AI use is often more reliable than these doctors for chronic conditions, preventions, diagnosis.
I wish your work reached a LOT more, both to doctors and general public. I wish more doctors have this curiosity and inclination. Please keep doing the great work.