
Air Pollution - What It Does To Our Hearts
On air pollution, cardiovascular disease, and the normalization of risk

When tech entrepreneur Bryan Johnson walked into Nikhil Kamath’s podcast studio in January, he came prepared. N95 mask on his face. Portable air purifier running beside him. Within an hour, he walked out midway through the recording.
The reason? Despite being inside a five-star hotel with his own filtration equipment, the indoor AQI measured 130, with PM2.5 at 75 μg/m³. “I can’t see you over there,” he told Kamath during the recording. By his third day in India, his skin had broken out in a rash. His eyes and throat burned. The room circulated outdoor air, rendering his purifier ineffective.
Johnson later wrote on X: “Inside, the AQI was 130 and PM2.5 was 75 μg/m³, which is equal to smoking 3.4 cigarettes for 24 hours of exposure.”
The internet split. Some mocked him for overreacting. Others questioned why he came to India at all.
But Johnson made an observation worth examining: “Air pollution has been so normalized in India that no one even notices anymore despite the science of its negative effects being well known.”
He’s not wrong. In November, thousands ran the Delhi Half Marathon while the city’s AQI exceeded 300—inhaling the equivalent of roughly 30 cigarettes during the race. People go for morning jogs when PM2.5 levels hit 200 μg/m³. Children play outside at recess regardless of air quality. The normalization is complete.
Johnson left after three days. Most people don’t have that option.
1. The invisible scar
We’ve known for years that air pollution causes heart disease. What we didn’t know until recently is that damage starts accumulating at pollution levels we’ve been calling “acceptable.”
A 2025 study in Radiology examined 694 patients using cardiac MRI and found something disturbing: for every 1 μg/m³ increase in long-term PM2.5 exposure, there was measurable diffuse myocardial fibrosis—essentially scarring of the heart muscle. This occurred even in healthy individuals without heart disease, and the relationship held at PM2.5 levels below current regulatory standards.
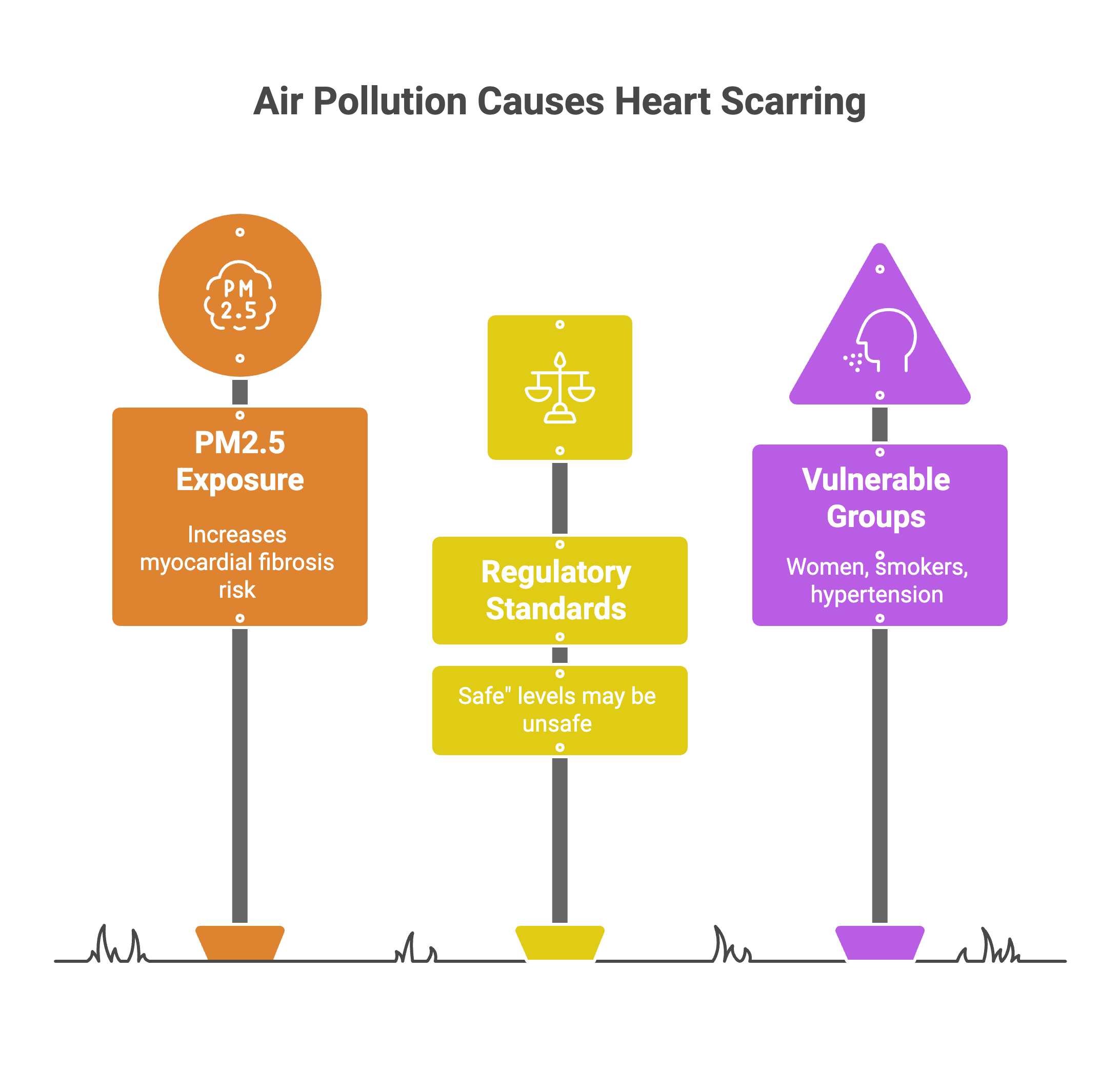
Delhi’s annual average PM2.5 ranges from 80-120 μg/m³. Residents breathing this air for years are accumulating structural heart damage that predicts future heart failure and arrhythmias. The scarring happens silently, years before the first symptom appears.
Current Indian standards allow annual PM2.5 averages up to 40 μg/m³. The MRI data found no safe threshold. Fibrosis accumulated at every exposure level measured.
2. The plastic in your plaque
While PM2.5 has dominated the pollution conversation, a newer threat has emerged from an unexpected source: the microscopic plastic particles saturating urban air.
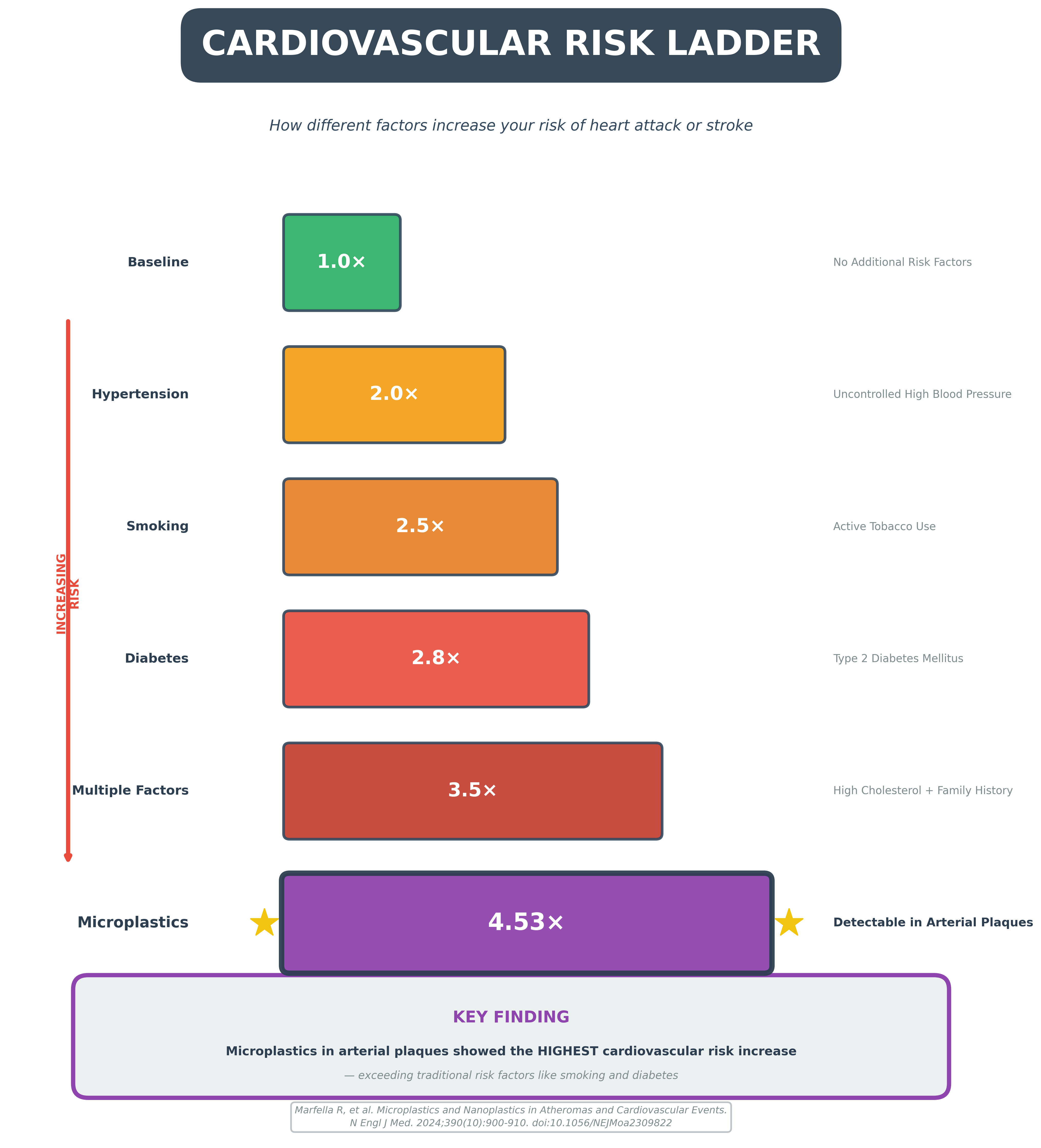
A 2024 study in the New England Journal of Medicine examined carotid artery plaques removed from 304 patients during endarterectomy. Researchers found polyethylene microplastics in 58.4% of samples and PVC in another 12.1%. Electron microscopy showed jagged-edged particles embedded within macrophages and scattered through plaque debris.
The clinical outcome was striking. Patients with detectable microplastics in their plaques faced a 4.53-fold increased risk of myocardial infarction, stroke, or death over 34 months of follow-up. Among the largest cardiovascular risk multipliers in recent literature.
These arterial microplastics enter the body primarily through ingestion - contaminated food, bottled water, and packaged products. But inhalation represents a second route. Recent studies by the Indian Institute of Tropical Meteorology found microplastics suspended in Delhi’s breathable air fractions: PM2.5 and PM1. Adults in Delhi inhale an estimated 1,935-5,621 microplastic particles annually. The composition matches what shows up in consumer products and urban waste: polyethylene terephthalate, polyethylene, polyester, polystyrene, and PVC.
The sources overlap with traditional air pollution. Tire abrasion releases polymer particles into PM2.5. Textile manufacturing and household laundry shed synthetic fibers. Plastic waste burning - common in unauthorized colonies - releases respirable microplastic particles. Delhi generates 1,145 tonnes of plastic waste daily, with 635 tonnes being single-use plastics.
Whether these inhaled particles reach arterial plaques, or whether the plaque burden reflects primarily ingested plastics, remains unclear. What’s established: microplastics trigger the same inflammatory mechanisms as PM2.5. Chronic inflammation. Oxidative stress. Endothelial dysfunction. They destabilize plaque and increase thrombotic risk. Unlike PM2.5, which the body can partially clear, microplastics persist indefinitely in tissues.
3. When pollution triggers heart attacks
The chronic effects of pollution—myocardial fibrosis and plastic-laden plaque—set the stage. Acute pollution spikes pull the trigger.
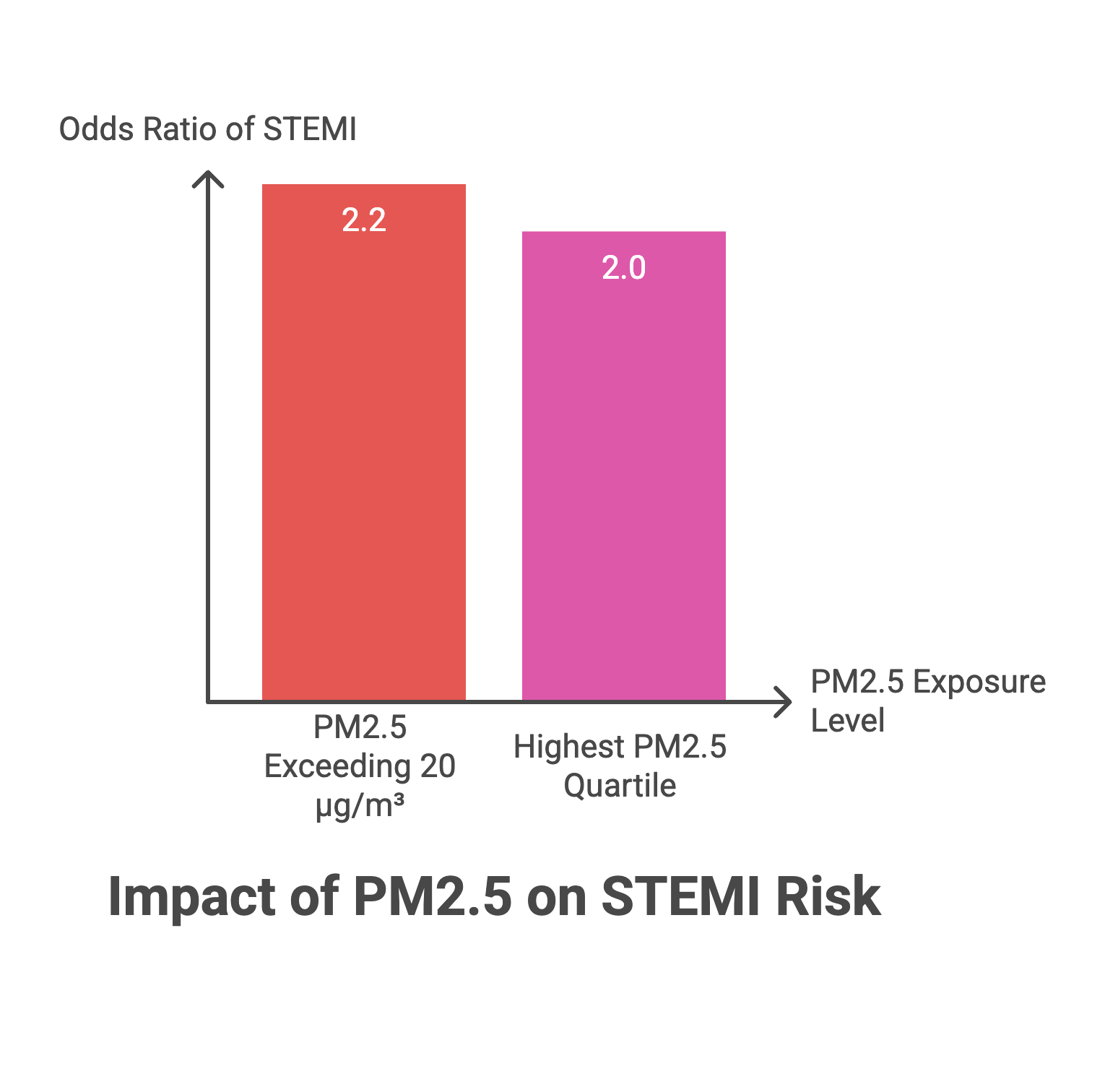
A 2024 case-crossover study from Argentina examined the relationship between wildfire-related PM2.5 spikes and ST-elevation myocardial infarctions. On days when PM2.5 exceeded 20 μg/m³, the odds of STEMI increased 2.2-fold. The risk climbed progressively with higher pollution quartiles. Residents exposed to the highest PM2.5 levels had double the STEMI risk compared to those breathing the cleanest air.
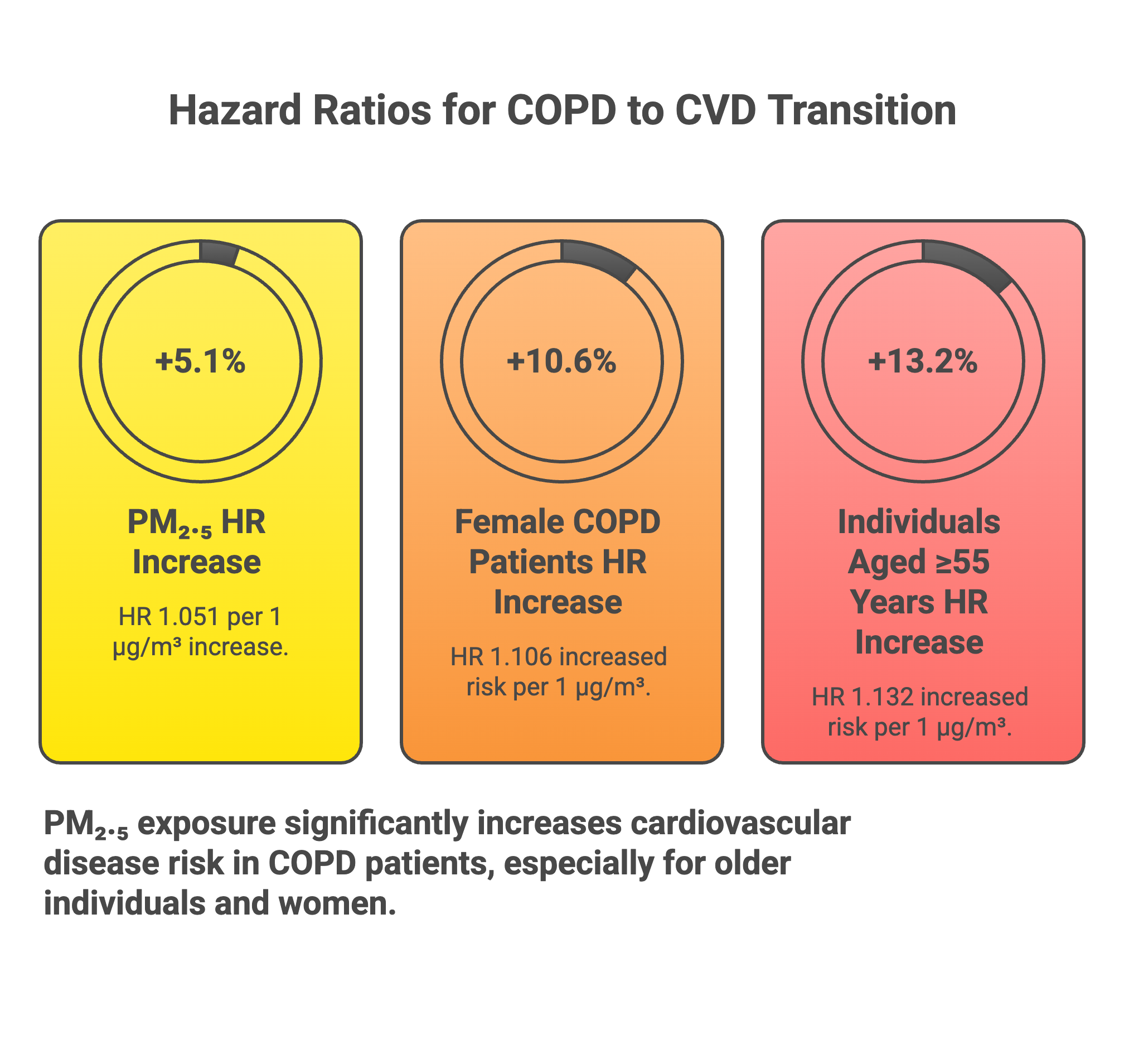
Delhi frequently records PM2.5 levels exceeding 200 μg/m³ during winter months, ten times the threshold where acute cardiac events spike. A comprehensive analysis in Ecotoxicology and Environmental Safety tracked 318,282 UK Biobank participants over 13.5 years. Among participants who developed COPD, each 1 μg/m³ increase in PM2.5 increased their subsequent risk of developing cardiovascular disease by 5.1%. The effect was strongest in women and those over 55 years old.
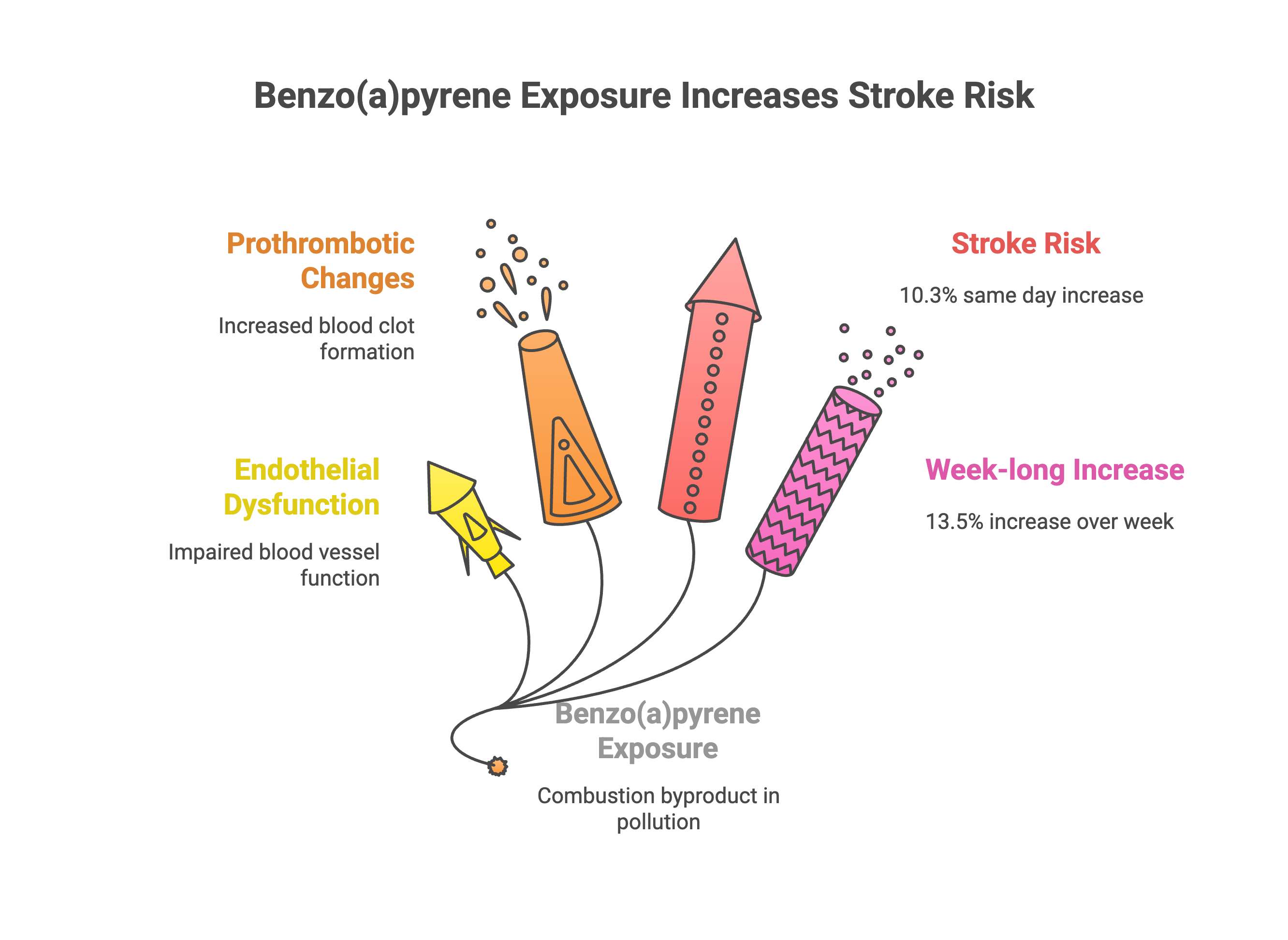
The temporal pattern matters. Research in Environmental Health examining ischemic stroke cases found that exposure to benzo(a)pyrene (a combustion byproduct common in pollution) increased stroke risk by 10.3% on the same day of exposure and 13.5% across a week-long window. The lag period suggests a cascade: pollution exposure triggers endothelial dysfunction and prothrombotic changes within hours, which manifest as acute events within days.
What’s actually happening at the cellular level? PM2.5 particles smaller than 2.5 micrometers penetrate deep into alveoli and enter the bloodstream. Within hours, these particles trigger oxidative stress, activate inflammatory pathways (particularly IL-6 and TNF-alpha), increase blood viscosity, and promote autonomic nervous system imbalance—shifting toward sympathetic dominance. The cumulative effect: unstable plaques rupture, coronary arteries spasm, and clots form more readily.
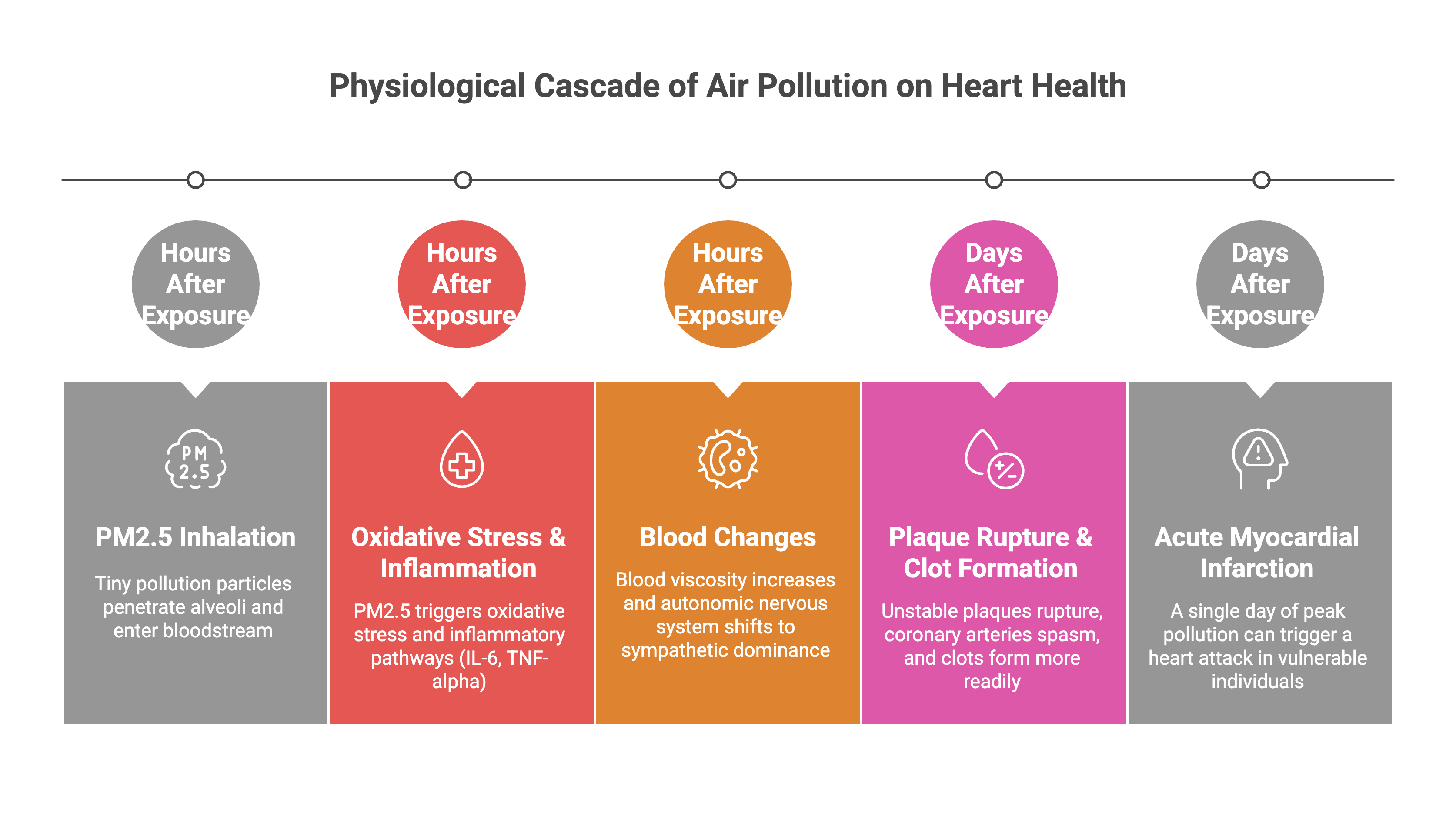
Patients with pre-existing plaques are especially vulnerable. A single day breathing Delhi’s peak pollution levels can convert decades of silent arterial disease into an acute myocardial infarction.
4. What you can do
The part you and I can control is exposure. Personal protective measures reduce exposure. They don’t eliminate risk.
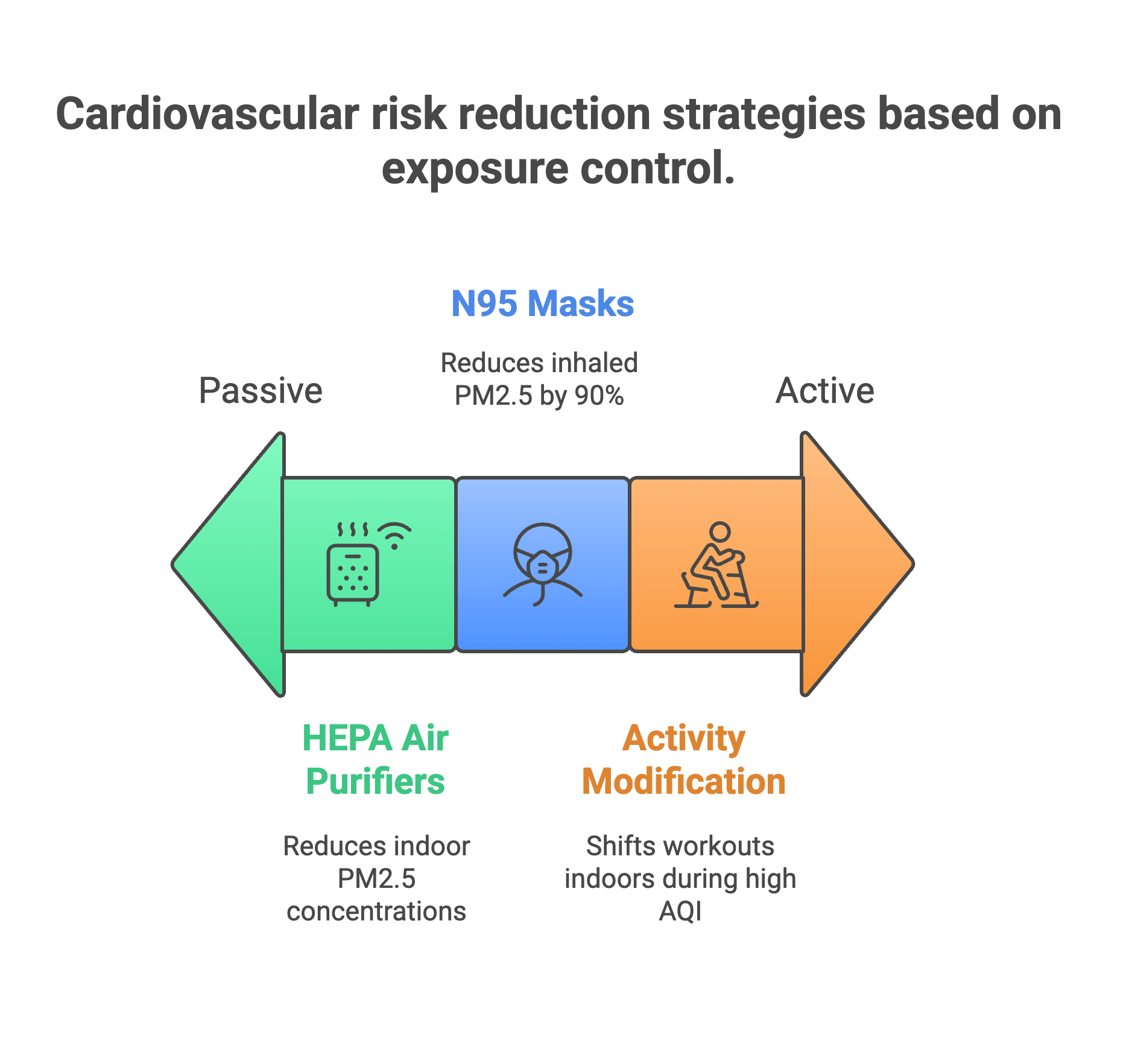
A 2020 American Heart Association scientific statement reviewed interventions against particulate matter. HEPA filtration reduced indoor PM2.5 by 58-65% in controlled studies. For people with elevated blood pressure, HEPA units lowered systolic readings by 2-3 mmHg—comparable to low-dose medication effects. N95 masks cut inhaled PM2.5 by 90% when properly fitted. These interventions work.
But they’re insufficient for people with established cardiovascular disease. A study tracking 73,425 U.S. veterans after percutaneous coronary intervention found that each 1 μg/m³ increase in annual PM2.5 exposure raised the risk of heart attack, stroke, or death by 8.7%. Patients exposed to 10 μg/m³ lost 1.1 months of life at five years compared to those breathing 5 μg/m³ air. By 15 years, the difference reached 7.6 months. Even at the relatively low PM2.5 levels in the United States, pollution shortened survival in this vulnerable population.
The post-PCI data matters because it represents patients under optimal medical therapy. Stents placed. Antiplatelet agents prescribed. Risk factors managed. Pollution still accelerated disease progression.
The exercise paradox compounds the problem. Physical inactivity causes cardiovascular disease. Exercise prevents it. But a 2021 European Heart Journal editorial summarized the evidence: exercise in clean air protects the heart, while exercise in polluted air causes harm. The ventilatory rate during exertion increases PM2.5 deposition deep in lung tissue. The cardiovascular benefits of movement don’t outweigh the inflammatory damage from inhaled particulates when air quality deteriorates past certain thresholds.
This creates an impossible choice. Avoid outdoor exercise and lose cardiovascular fitness. Exercise outdoors and accelerate atherosclerosis. Neither option is acceptable.
You’ll hear recommendations about antioxidant supplements. Vitamins C and E. Fish oil. Olive oil. A 2016 review in Biochimica et Biophysica Acta suggested these might protect against short-term pollution exposure by reducing oxidative stress. The hypothesis sounds reasonable.
The clinical trial data tell a different story. Large randomized trials testing antioxidant vitamins for cardiovascular disease prevention have consistently failed. HOPE trial, GISSI trial, Heart Protection Study—vitamin E showed no benefit. Vitamin C showed no benefit. The observational studies showing protective associations were confounded by healthier baseline characteristics in supplement users. People who take vitamins also eat better, exercise more, and see doctors regularly. The supplements weren’t protecting them. Their overall health behaviors were.
Fish oil trials produce similar results. STRENGTH trial, ASCEND trial—no reduction in cardiovascular events. The omega-3 fatty acids that appear protective in observational nutrition studies don’t translate to benefit when isolated in pill form and tested rigorously.
Supplementation won’t counteract chronic pollution exposure. The inflammatory and oxidative stress pathways activated by PM2.5 and microplastics operate at a scale that overwhelms what dietary antioxidants can neutralize.
Personal protective equipment and behavior modification provide marginal risk reduction. For someone breathing heavily polluted air year after year, filtration and masking decrease exposure by perhaps 50-70% during the hours spent indoors or masked. The remaining exposure continues accumulating cardiovascular damage.
The solution isn’t individual. It’s regulatory. Air quality standards need tightening. Enforcement needs strengthening. The evidence showing no safe threshold for PM2.5 exposure argues for pursuing the lowest achievable concentrations, not compromising at levels convenient for industry.
Until that happens, the interventions worth implementing: HEPA filtration in living and sleeping spaces. N95 masks during peak pollution periods. Checking air quality before outdoor exercise and canceling when readings exceed safe levels. Avoiding prolonged outdoor exposure on high pollution days.
But understand what these measures accomplish. They reduce exposure. They don’t restore the cardiovascular health that would exist under clean air. None of this is a cure for the city’s air, and policy will always dwarf personal tactics.
If you found this useful, please share it.
Evidence over opinions. Clarity over noise. That’s Signal Over Noise.
References
All evidence in this newsletter derives from peer-reviewed studies published in leading medical journals. DOI links to original articles are provided for verification.
Myocardial Fibrosis and Chronic Exposure:
Association between Long-term Exposure to Ambient Air Pollution and Myocardial Fibrosis Assessed with Cardiac MRI. Radiology 2025. https://doi.org/10.1148/radiol.250331
Microplastics and Cardiovascular Disease:
Marfella R, et al. Microplastics and Nanoplastics in Atheromas and Cardiovascular Events. New England Journal of Medicine 2024. https://doi.org/10.1056/NEJMoa2309822
Acute Cardiovascular Events:
Impact of wildfires and PM2.5 on ST-elevation acute coronary syndrome in Rosario City, Argentina. International Journal of Environmental Health Research 2024. https://doi.org/10.1080/09603123.2024.2434208
Dynamic associations between long-term exposure to ambient air pollution and respiratory-cardiovascular diseases: A trajectory analysis. Ecotoxicology and Environmental Safety 2025. https://doi.org/10.1016/j.ecoenv.2025.119329
Short-term exposure to air pollution and risk of ischemic stroke requiring intravenous thrombolysis. Environmental Health 2025. https://doi.org/10.1186/s12940-025-01230-2
Vulnerable Populations:
Motairek I, et al. Particulate Matter Air Pollution and Long-Term Outcomes in Patients Undergoing Percutaneous Coronary Intervention. JACC Advances 2023. https://doi.org/10.1016/j.jacadv.2023.100285
Warburton DER, et al. A Systematic Review of the Short-Term Health Effects of Air Pollution in Persons Living with Coronary Heart Disease. Journal of Clinical Medicine 2019. https://doi.org/10.3390/jcm8020274
Exercise and Air Pollution:
Münzel T, Hahad O, Daiber A. Running in polluted air is a two-edged sword. European Heart Journal 2021. https://doi.org/10.1093/eurheartj/ehab227
Personal Protective Measures:
Rajagopalan S, et al. Personal-Level Protective Actions Against Particulate Matter Air Pollution Exposure: A Scientific Statement From the American Heart Association. Circulation 2020. https://doi.org/10.1161/CIR.0000000000000931
Dietary Interventions:
Tong H. Dietary and pharmacological intervention to mitigate the cardiopulmonary effects of air pollution toxicity. Biochimica et Biophysica Acta 2016. https://doi.org/10.1016/j.bbagen.2016.05.014